

Is it safe to delay appendectomy in adults with acute appendicitis?
- PMID: 17060754
- PMCID: PMC1856602
- DOI: 10.1097/01.sla.0000231726.53487.dd
Is it safe to delay appendectomy in adults with acute appendicitis?
Abstract
Objective: To examine whether delayed surgical intervention in adult patients with acute appendicitis is safe by correlating the interval from onset of symptoms to operation (total interval) with the degree of pathology and incidence of postoperative complications.
Summary background data: Prompt appendectomy has long been the standard of care for acute appendicitis because of the risk of progression to advanced pathology. This time-honored practice has been recently challenged by studies in pediatric patients, which suggested that acute appendicitis can be managed in an elective manner once antibiotic therapy is initiated. No such data are available in adult patients with acute appendicitis.
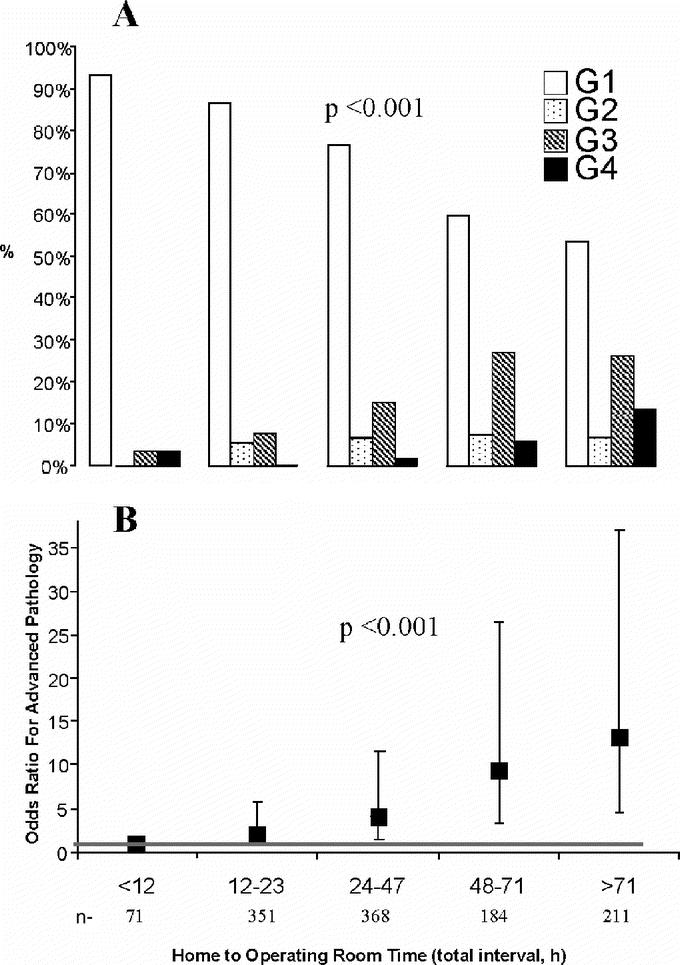
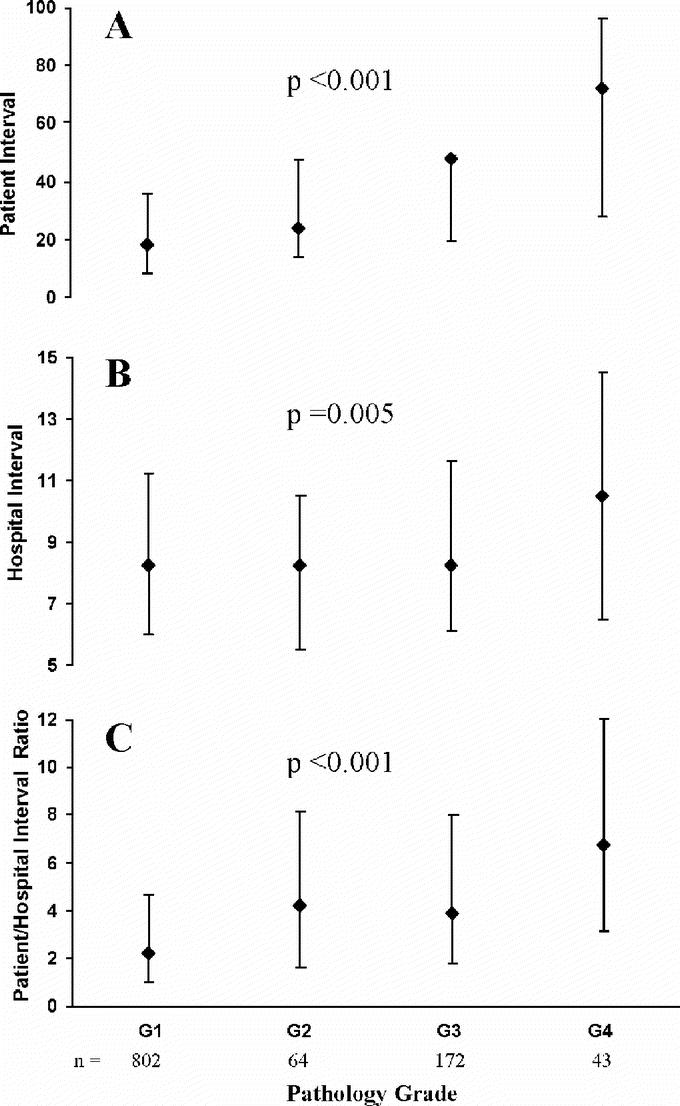
Methods: A retrospective review of 1081 patients who underwent an appendectomy for acute appendicitis between 1998 and 2004 was conducted. The following parameters were monitored and correlated: demographics, time from onset of symptoms to arrival at the emergency room (patient interval) and from arrival to the emergency room to the operating room (hospital interval), physical, computed tomography (CT scan) and pathologic findings, complications, length of stay, and length of antibiotic treatment. Pathologic state was graded 1 (G1) for acute appendicitis, 2 (G2) for gangrenous acute appendicitis, 3 (G3) for perforation or phlegmon, and 4 (G4) for a periappendicular abscess.
Results: The risk of advanced pathology, defined as a higher pathology grade, increased with the total interval. When this interval was <12 hours, the risk of developing G1, G2, G3, and G4, was 94%, 0%, 3%, and 3%, respectively. These values changed to 60%, 7%, 27%, and 6%, respectively, when the total interval was 48 to 71 hours and to 54%, 7%, 26%, and 13% for longer than 71 hours. The odds for progressive pathology was 13 times higher for the total interval >71 hours group compared with total interval<12 hours (95% confidence interval = 4.7-37.1). Although both prolonged patient and hospital intervals were associated with advanced pathology, prehospital delays were more profoundly related to worsening pathology compared with in-hospital delays (P < 0.001). Advanced pathology was associated with tenderness to palpation beyond the right lower quadrant (P < 0.001), guarding (P < 0.001), rebound (P < 0.001), and CT scan findings of peritoneal fluid (P = 0.01), fecalith (P = 0.01), dilation of the appendix (P < 0.001), and perforation (P < 0.001). Increased length of hospital stay (P < 0.001) and antibiotic treatment (P < 0.001) as well as postoperative complications (P < 0.001) also correlated with progressive pathology.
Conclusion: In adult patients with acute appendicitis, the risk of developing advanced pathology and postoperative complications increases with time; therefore, delayed appendectomy is unsafe. As delays in seeking medical help are difficult to control, prompt appendectomy is mandatory. Because these conclusions are derived from retrospective data, a prospective study is required to confirm their validity.
Figures
Comment in
-
Appendicitis 2006.Ann Surg. 2006 Nov;244(5):661-2. doi: 10.1097/01.sla.0000243591.65502.02. Ann Surg. 2006. PMID: 17060755 Free PMC article. No abstract available.
References
-
- Owings MF, Kozak LJ. Ambulatory and in-patient procedures in the United States, 1996. In: Vital and Health Statistics, Series 13, No. 139 [DHHS publication no. (PHS) 99-1710.] Hyattsville, MD: National Center for Health Statistics, 1998:26. - PubMed
-
- Yardeni D, Hirschl RB. Delayed versus immediate surgery in acute appendicitis: do we need to operate in the middle of the night? J Pediatr Surg. 2004;39:464–469. - PubMed
-
- Bachoo P, Mahomed AA, Ninan GK, et al. Acute appendicitis: the continuing role for active observation. Pediatr Surg Int. 2001;17:125–138. - PubMed
-
- Hosmer DW, Lemeshow S. Applied Logistic Regression, 2nd ed. New York: John Wiley and Sons, 2000:288–308.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
