

Screening strategies for chronic kidney disease in the general population: follow-up of cross sectional health survey
- PMID: 17062598
- PMCID: PMC1647344
- DOI: 10.1136/bmj.39001.657755.BE
Screening strategies for chronic kidney disease in the general population: follow-up of cross sectional health survey
Abstract
Objective: To find an effective screening strategy for detecting patients with chronic kidney disease and to describe the natural course of the disease.
Design: Eight year follow-up of a cross sectional health survey (the HUNT II study).
Setting: Nord-Trøndelag County, Norway
Participants: 65,604 people (70.6 % of all adults aged >or=20 in the county).
Main outcome measures: Incident end stage renal disease (ESRD) and cardiovascular mortality monitored by individual linkage to central registries.
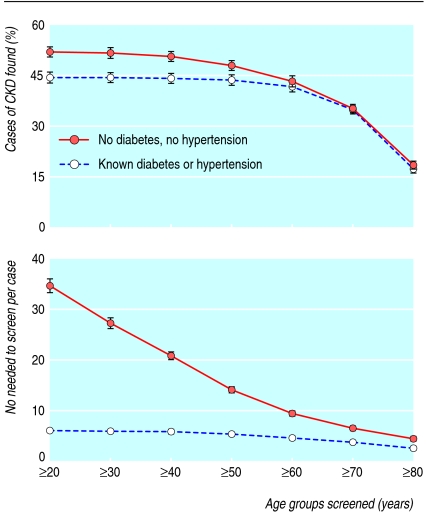
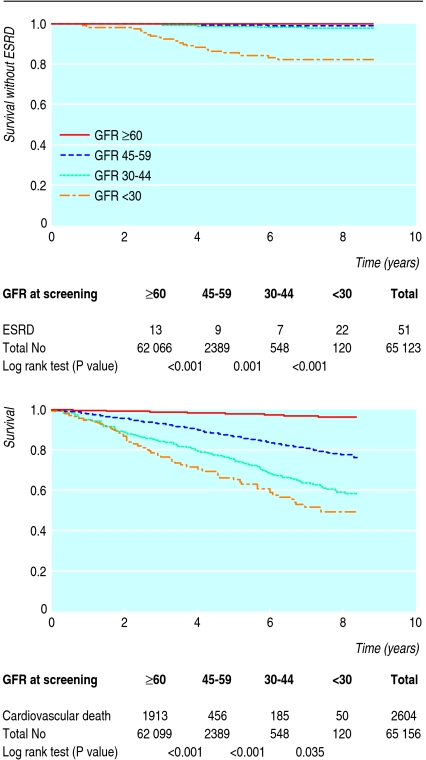
Results: 3069/65,604 (4.7%) people had chronic kidney disease (estimated glomerular filtration rate <60 ml/min/1.73 m(2)), so we would need to screen 20.6 people (95% confidence interval 20.0 to 21.2) to identify one case. Restriction of screening to those with hypertension, diabetes, or age >55 would identify 93.2% (92.4% to 94.0%) of patients with chronic kidney disease, with a number needed to screen of 8.7 (8.5 to 9.0). Restriction of screening according to guidelines of the United States kidney disease outcomes quality initiative (US KDOQI) gave similar results, but restriction according to the United Kingdom's chronic kidney disease guidelines detected only 60.9% (59.1% to 62.8%) of cases. Screening only people with previously known diabetes or hypertension detected 44.2% (42.7% to 45.7%) of all cases, with a number needed to screen of six. During the eight year follow-up only 38 of the 3069 people with chronic kidney disease progressed to end stage renal disease, and the risk was especially low in people without diabetes or hypertension, women, and those aged >or=70 or with a glomerular filtration rate 45-59 ml/min/1.73 m(2) at screening. In contrast, there was a high cardiovascular mortality: 3.5, 7.4, and 10.1 deaths per 100 person years among people with a glomerular filtration rate 45-59, 30-44, and <30 ml/min/1.73 m(2), respectively.
Conclusion: Screening people with hypertension, diabetes mellitus, or age >55 was the most effective strategy to detect patients with chronic kidney disease, but the risk of end stage renal disease among those detected was low.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Glomerular filtration rate: screening cannot be recommended on the basis of current knowledge.BMJ. 2006 Nov 18;333(7577):1030-1. doi: 10.1136/bmj.39030.594259.BE. BMJ. 2006. PMID: 17110701 Free PMC article. No abstract available.
References
-
- van Dijk PC, Jager KJ, de Charro F, Collart F, Cornet R, Dekker FW, et al. Renal replacement therapy in Europe: the results of a collaborative effort by the ERA-EDTA registry and six national or regional registries. Nephrol Dial Transplant 2001;16:1120-9. - PubMed
-
- US Renal Data System/National Institutes of Health. Annual data report: atlas of end-stage renal disease in the United States. 2003. www.usrds.org/adr.htm (accessed May 2004).
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 2004;351:1296-305. - PubMed
-
- Henry RM, Kostense PJ, Bos G, Dekker JM, Nijpels G, Heine RJ, et al. Mild renal insufficiency is associated with increased cardiovascular mortality: the Hoorn study. Kidney Int 2002;62:1402-7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical