

Responsiveness and minimal clinically important difference for pain and disability instruments in low back pain patients
- PMID: 17064410
- PMCID: PMC1635558
- DOI: 10.1186/1471-2474-7-82
Responsiveness and minimal clinically important difference for pain and disability instruments in low back pain patients
Abstract
Background: The choice of an evaluative instrument has been hampered by the lack of head-to-head comparisons of responsiveness and the minimal clinically important difference (MCID) in subpopulations of low back pain (LBP). The objective of this study was to concurrently compare responsiveness and MCID for commonly used pain scales and functional instruments in four subpopulations of LBP patients.
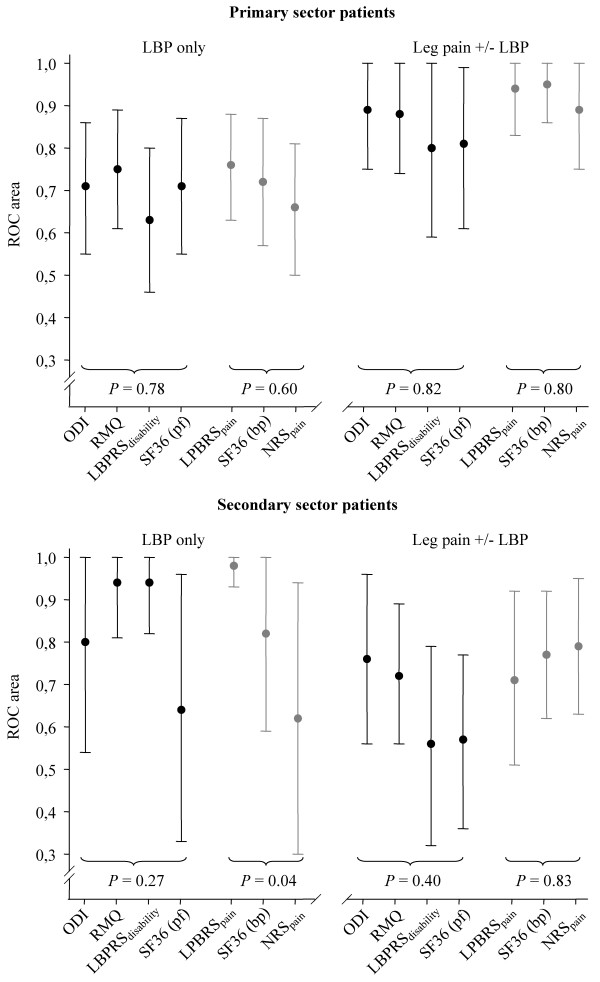
Methods: The Danish versions of the Oswestry Disability Index (ODI), the 23-item Roland Morris Disability Questionnaire (RMQ), the physical function and bodily pain subscales of the SF36, the Low Back Pain Rating Scale (LBPRS) and a numerical rating scale for pain (0-10) were completed by 191 patients from the primary and secondary sectors of the Danish health care system. Clinical change was estimated using a 7-point transition question and a numeric rating scale for importance. Responsiveness was operationalized using standardized response mean (SRM), area under the receiver operating characteristic curve (ROC), and cut-point analysis. Subpopulation analyses were carried out on primary and secondary sector patients with LBP only or leg pain +/- LBP.
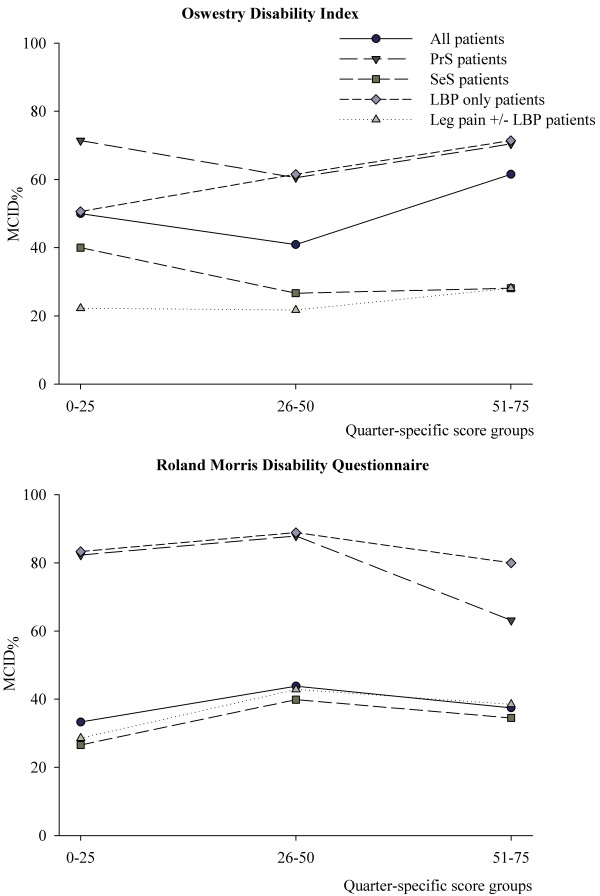
Results: RMQ was the most responsive instrument in primary and secondary sector patients with LBP only (SRM = 0.5-1.4; ROC = 0.75-0.94) whereas ODI and RMQ showed almost similar responsiveness in primary and secondary sector patients with leg pain (ODI: SRM = 0.4-0.9; ROC = 0.76-0.89; RMQ: SRM = 0.3-0.9; ROC = 0.72-0.88). In improved patients, the RMQ was more responsive in primary and secondary sector patients and LBP only patients (SRM = 1.3-1.7) while the RMQ and ODI were equally responsive in leg pain patients (SRM = 1.3 and 1.2 respectively). All pain measures demonstrated almost equal responsiveness. The MCID increased with increasing baseline score in primary sector and LBP only patients but was only marginally affected by patient entry point and pain location. The MCID of the percentage change score remained constant for the ODI (51%) and RMQ (38%) specifically and differed in the subpopulations.
Conclusion: RMQ is suitable for measuring change in LBP only patients and both ODI and RMQ are suitable for leg pain patients irrespectively of patient entry point. The MCID is baseline score dependent but only in certain subpopulations. Relative change measured using the ODI and RMQ was not affected by baseline score when patients quantified an important improvement.
Figures
Similar articles
-
Danish version of the Oswestry disability index for patients with low back pain. Part 2: Sensitivity, specificity and clinically significant improvement in two low back pain populations.Eur Spine J. 2006 Nov;15(11):1717-28. doi: 10.1007/s00586-006-0128-6. Epub 2006 May 31. Eur Spine J. 2006. PMID: 16736202
-
Danish version of the Oswestry Disability Index for patients with low back pain. Part 1: Cross-cultural adaptation, reliability and validity in two different populations.Eur Spine J. 2006 Nov;15(11):1705-16. doi: 10.1007/s00586-006-0117-9. Epub 2006 May 31. Eur Spine J. 2006. PMID: 16736204
-
Outcome measures in chronic low back pain.Eur Spine J. 2010 Sep;19(9):1484-94. doi: 10.1007/s00586-010-1353-6. Epub 2010 Apr 17. Eur Spine J. 2010. PMID: 20397032 Free PMC article.
-
Predictors of success of pharmacological management in patients with chronic lower back pain: systematic review.J Orthop Surg Res. 2024 Apr 18;19(1):248. doi: 10.1186/s13018-024-04741-9. J Orthop Surg Res. 2024. PMID: 38637804 Free PMC article.
-
Meta-analysis identifies Back Pain Questionnaire reliability influenced more by instrument than study design or population.J Clin Epidemiol. 2013 Mar;66(3):261-7. doi: 10.1016/j.jclinepi.2012.06.024. J Clin Epidemiol. 2013. PMID: 23347850 Review.
Cited by
-
Surgery versus nonsurgical treatment of lumbar spinal stenosis: a randomized trial.Ann Intern Med. 2015 Apr 7;162(7):465-73. doi: 10.7326/M14-1420. Ann Intern Med. 2015. PMID: 25844995 Free PMC article. Clinical Trial.
-
Postoperative lordosis distribution index, patient reported outcome measures, and revision surgery following transforaminal lumbar interbody fusion.World Neurosurg X. 2023 Dec 12;21:100251. doi: 10.1016/j.wnsx.2023.100251. eCollection 2024 Jan. World Neurosurg X. 2023. PMID: 38173686 Free PMC article.
-
General health factors may be a barrier to effective non-surgical multidisciplinary rehabilitation of common orthopaedic conditions in tertiary care settings.BMC Musculoskelet Disord. 2018 Sep 27;19(1):348. doi: 10.1186/s12891-018-2265-6. BMC Musculoskelet Disord. 2018. PMID: 30261861 Free PMC article.
-
Similar improvements in patient-reported outcomes for non-specific low back pain patients with and without lumbar spinal stenosis symptoms following a structured education and exercise therapy program.BMC Musculoskelet Disord. 2023 Oct 25;24(1):839. doi: 10.1186/s12891-023-06950-5. BMC Musculoskelet Disord. 2023. PMID: 37880624 Free PMC article.
-
Estimating the number needed to treat from continuous outcomes in randomised controlled trials: methodological challenges and worked example using data from the UK Back Pain Exercise and Manipulation (BEAM) trial.BMC Med Res Methodol. 2009 Jun 11;9:35. doi: 10.1186/1471-2288-9-35. BMC Med Res Methodol. 2009. PMID: 19519911 Free PMC article.
References
-
- Streiner DL, Norman GR. In: Health Measurment Scales A Practical Guide to Their Development and Use. Third. Streiner DL and Norman GR, editor. Oxford, Oxford Medical Publications; 2003.
-
- Grotle M, Brox JI, Vollestad NK. Functional Status and Disability Questionnaires: What Do They Assess?: A Systematic Review of Back-Specific Outcome Questionnaires. Spine. 2005;30:130–140. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
