

Natural history of a randomized trial comparing distal spleno-renal shunt with endoscopic sclerotherapy in the prevention of variceal rebleeding: a lesson from the past
- PMID: 17072957
- PMCID: PMC4088142
- DOI: 10.3748/wjg.v12.i39.6331
Natural history of a randomized trial comparing distal spleno-renal shunt with endoscopic sclerotherapy in the prevention of variceal rebleeding: a lesson from the past
Abstract
Aim: To compare endoscopic sclerotherapy (ES) with distal splenorenal shunt (DSRS) in the prevention of recurrent variceal bleeding in cirrhotic patients during a long-term follow-up period.
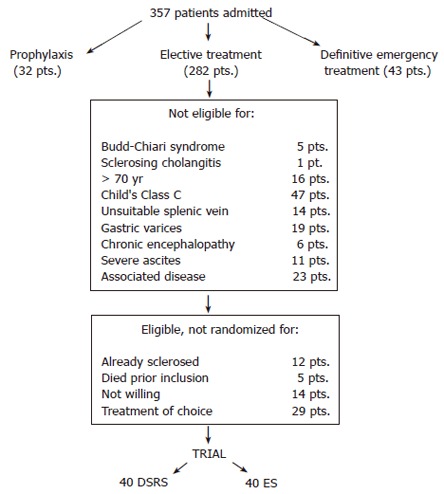
Methods: In 1984 we started a prospective, controlled study of patients with liver cirrhosis. Long-term follow-up presents a natural history of liver cirrhosis complicated by advanced portal hypertension. In this study the effects of 2 types of treatment, DSRS or ES, were evaluated. The study population included 80 patients with cirrhosis and portal hypertension referred to our department from October 1984 to March 1991. These patients were drawn from a pool of 282 patients who underwent either elective surgery or ES during the same period of time. Patients were assigned to one of the 2 groups according to a random number table: 40 to DSRS and 40 to ES using polidocanol.
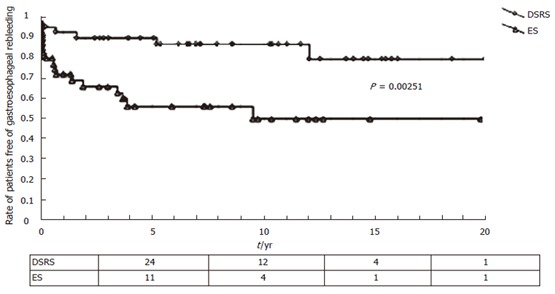
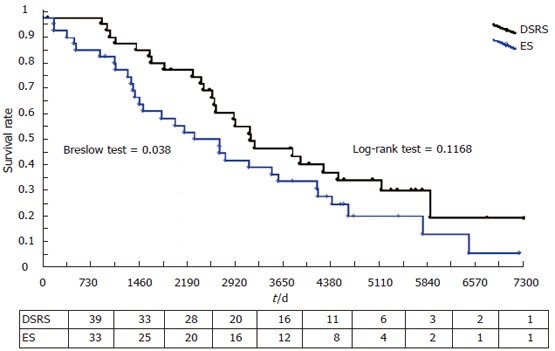
Results: During the postoperative period, no DSRS patient died, while one ES patient died of uncontrolled hemorrhage. One DSRS patient had mild recurrent variceal hemorrhage despite an angiographically patent DSRS and another patient suffered duodenal ulcer rebleeding. Eight ES patients suffered at least one episode of gastrointestinal bleeding: 4 from varices and 4 from esophageal ulcerations. Eight ES patients developed transitory dysphagia. Long-term follow-up was completed in all patients except for 5 cases (2 DSRS and 3 ES patients). Five-year survival rates for shunt (73%) and ES (56%) groups were statistically different: in this follow-up period and in subsequent follow-ups this difference decreased and ceased to be of statistical relevance. The primary cause of death became hepatocellular carcinoma (HCC). Four DSRS patients rebled due to duodenal ulcer, while eleven ES patients had recurrent bleeding from esophago-gastric sources (seven from varices, three from hypertensive gastropathy, one from esophageal ulcerations) and two from unknown sources. Nine DSRS and 2 ES patients developed a chronic encephalopathy; 13 DSRS and 5 ES patients suffered at least one episode of acute encephalopathy. Five ES patients had esophageal stenoses, which were successfully dilated.
Conclusion: In a subgroup of patients with good liver function, DSRS with a correct portal-azygos disconnection more effectively prevents variceal rebleeding than ES. However, this positive effect did not influence the long-term survival because other factors (e.g. HCC) were more important in deciding the fate of the cirrhotic patients with portal hypertension.
Figures
References
-
- Henderson JM, Millikan WJ, Warren WD. The distal splenorenal shunt: an update. World J Surg. 1984;8:722–732. - PubMed
-
- Spina GP, Galeotti F, Opocher E, Santambrogio R, Cucchiaro G, Lopez C, Pezzuoli G. Selective distal splenorenal shunt versus side-to-side portacaval shunt. Clinical results of a prospective, controlled study. Am J Surg. 1988;155:564–571. - PubMed
-
- Henderson JM, Kutner MH, Millikan WJ Jr, Galambos JT, Riepe SP, Brooks WS, Bryan FC, Warren WD. Endoscopic variceal sclerosis compared with distal splenorenal shunt to prevent recurrent variceal bleeding in cirrhosis. A prospective, randomized trial. Ann Intern Med. 1990;112:262–269. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
