

Post-operative atrial fibrillation is influenced by beta-blocker therapy but not by pre-operative atrial cellular electrophysiology
- PMID: 17074009
- PMCID: PMC2518219
- DOI: 10.1111/j.1540-8167.2006.00592.x
Post-operative atrial fibrillation is influenced by beta-blocker therapy but not by pre-operative atrial cellular electrophysiology
Abstract
Introduction: We investigated whether post-cardiac surgery (CS) new-onset atrial fibrillation (AF) is predicted by pre-CS atrial cellular electrophysiology, and whether the antiarrhythmic effect of beta-blocker therapy may involve pre-CS pharmacological remodeling.
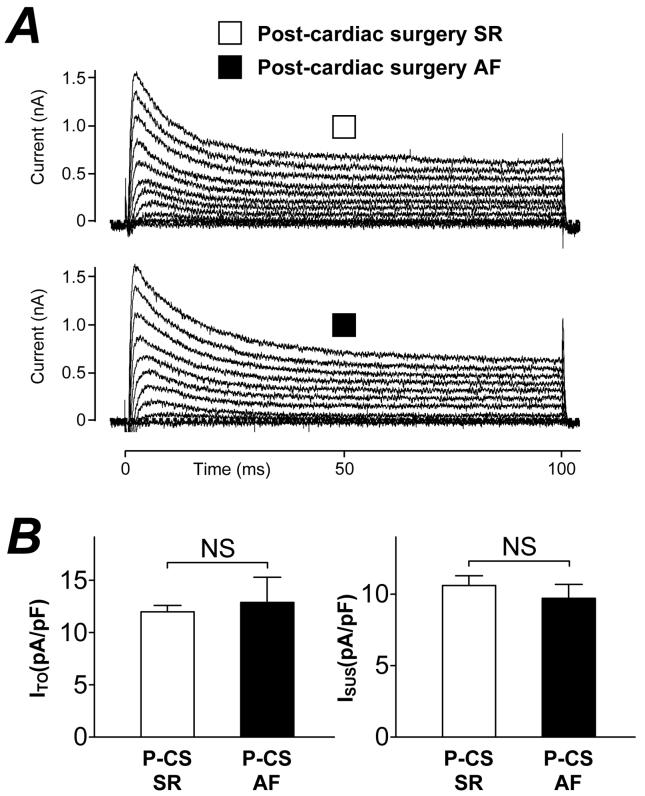
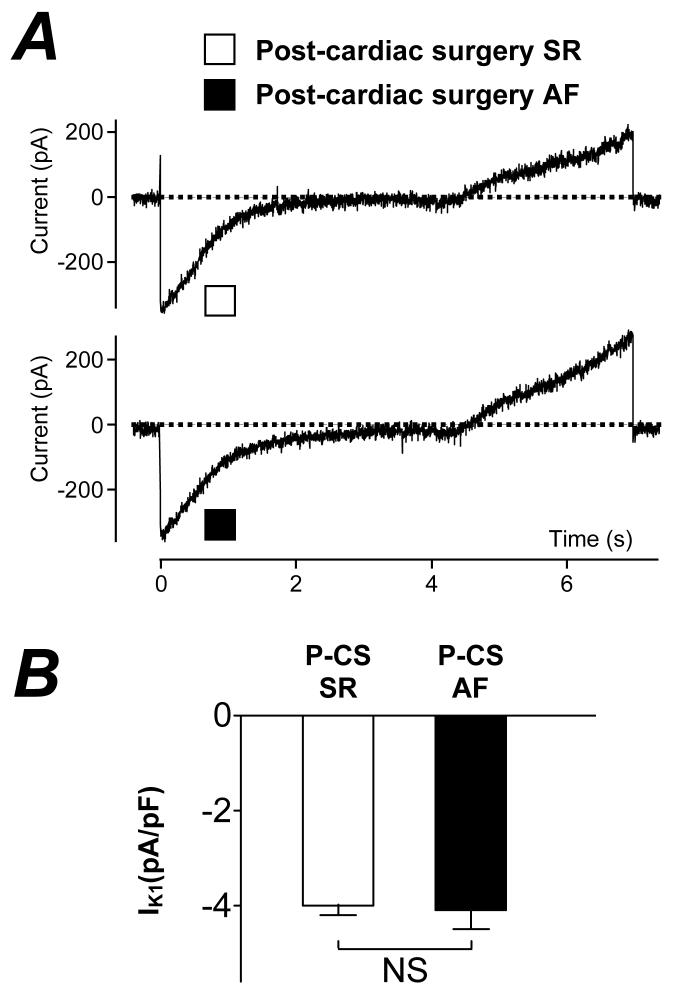
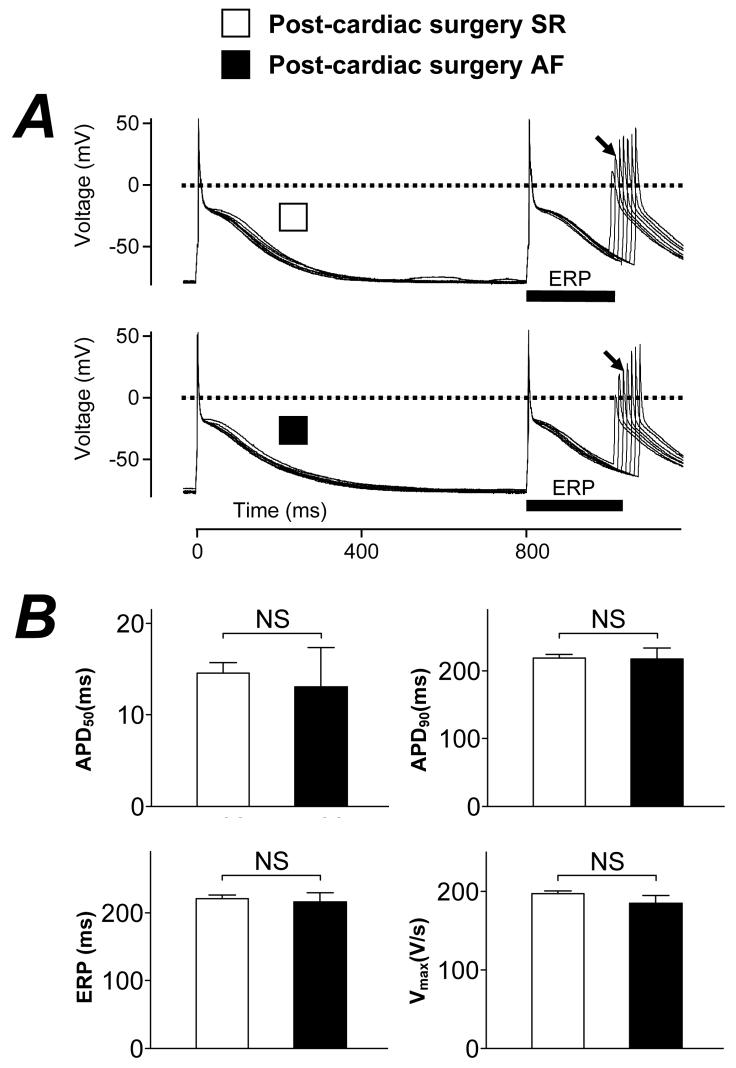
Methods and results: Atrial myocytes were obtained from consenting patients in sinus rhythm, just prior to CS. Action potentials and ion currents were recorded using whole-cell patch-clamp technique. Post-CS AF occurred in 53 of 212 patients (25%). Those with post-CS AF were older than those without (67 +/- 2 vs 62 +/- 1 years, P = 0.005). In cells from patients with post-CS AF, the action potential duration at 50% and 90% repolarization, maximum upstroke velocity, and effective refractory period (ERP) were 13 +/- 4 ms, 217 +/- 16 ms, 185 +/- 10 V/s, and 216 +/- 14 ms, respectively (n = 30 cells, 11 patients). Peak L-type Ca(2+) current, transient outward and inward rectifier K(+) currents, and the sustained outward current were -5.0 +/- 0.5, 12.9 +/- 2.4, -4.1 +/- 0.4, and 9.7 +/- 1.0 pA/pF, respectively (13-62 cells, 7-19 patients). None of these values were significantly different in cells from patients without post-CS AF (P > 0.05 for each, 60-279 cells, 29-86 patients), confirmed by multiple and logistic regression. In patients treated >7 days with a beta-blocker pre-CS, the incidence of post-CS AF was lower than in non-beta-blocked patients (13% vs 27%, P = 0.038). Pre-CS beta-blockade was associated with a prolonged pre-CS atrial cellular ERP (P = 0.001), by a similar degree (approximately 20%) in those with and without post-CS AF.
Conclusion: Pre-CS human atrial cellular electrophysiology does not predict post-CS AF. Chronic beta-blocker therapy is associated with a reduced incidence of post-CS AF, unrelated to a pre-CS ERP-prolonging effect of this treatment.
Figures

 , −BB, n=13/48) and treated (
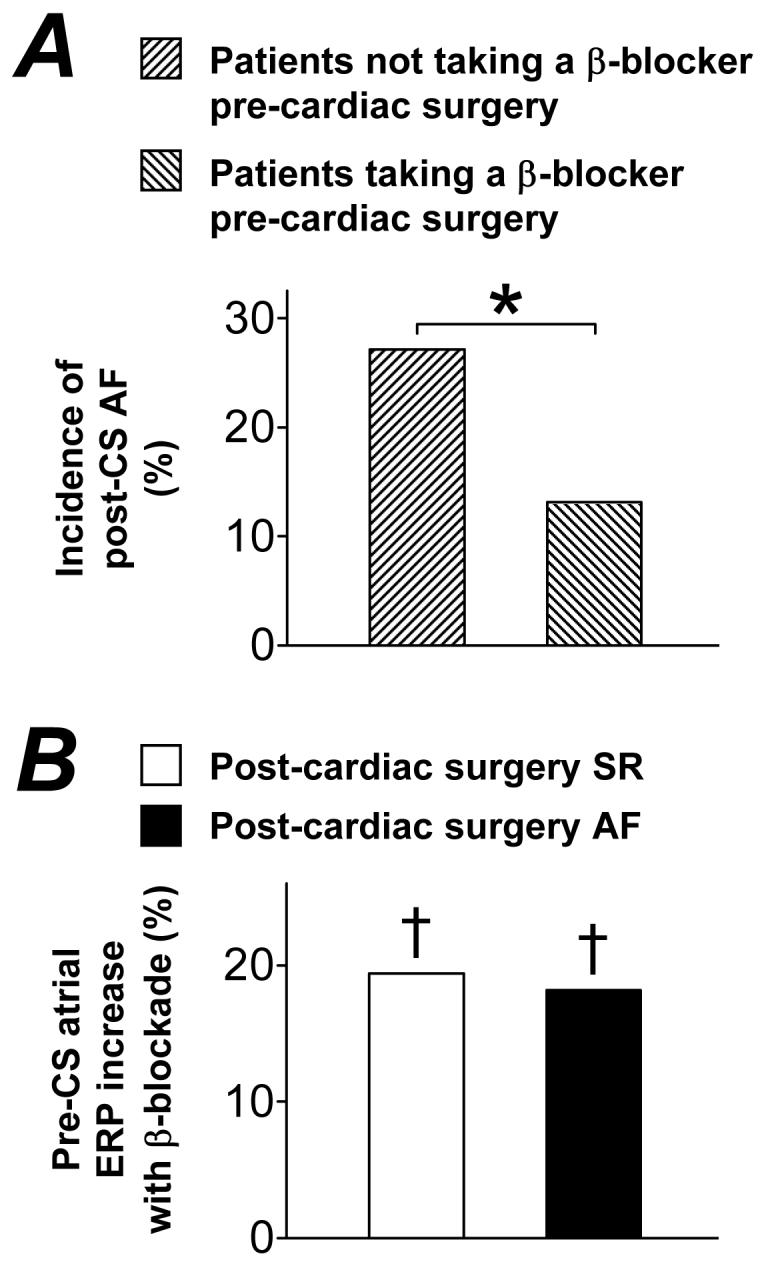
, −BB, n=13/48) and treated ( , +BB, n=13/99), respectively, for >7 days pre-CS with a beta-blocker. Asterisk denotes P<0.05 between groups. B, Comparison of magnitude of increase in mean pre-CS atrial cellular effective refractory period (ERP) associated with pre-CS treatment (>7 days) of patients with a beta-blocker, between those in post-CS sinus rhythm (□; patient n: −BB=21; +BB=43) and post (3 day)-CS AF (■; patient n: −BB=4; +BB=5). †s denote P<0.05 for the increase in ERP associated with pre-CS β-blockade within each group.
, +BB, n=13/99), respectively, for >7 days pre-CS with a beta-blocker. Asterisk denotes P<0.05 between groups. B, Comparison of magnitude of increase in mean pre-CS atrial cellular effective refractory period (ERP) associated with pre-CS treatment (>7 days) of patients with a beta-blocker, between those in post-CS sinus rhythm (□; patient n: −BB=21; +BB=43) and post (3 day)-CS AF (■; patient n: −BB=4; +BB=5). †s denote P<0.05 for the increase in ERP associated with pre-CS β-blockade within each group.Comment in
-
Preoperative atrial cardiomyocyte ionic currents and postoperative AF: important insights into what is not the mechanism.J Cardiovasc Electrophysiol. 2006 Nov;17(11):1239-41. doi: 10.1111/j.1540-8167.2006.00625.x. Epub 2006 Sep 21. J Cardiovasc Electrophysiol. 2006. PMID: 16995887 No abstract available.
References
-
- Mathew JP, Fontes ML, Tudor IC, Ramsay J, Duke P, Mazer CD, Barash PG, Hsu PH, Mangano DT. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA. 2004;291:1720–1729. - PubMed
-
- Villareal RP, Hariharan R, Liu BC, Kar B, Lee VV, Elayda M, Lopez JA, Rasekh A, Wilson JM. Massumi A: Postoperative atrial fibrillation and mortality after coronary artery bypass surgery. J Am Coll Cardiol. 2004;43:742–748. - PubMed
-
- Gang Y, Hnatkova K, Mandal K, Ghuran A, Malik M. Preoperative electrocardiographic risk assessment of atrial fibrillation after coronary artery bypass grafting. J Cardiovasc Electrophysiol. 2004;15:1379–1386. - PubMed
-
- Dobrev D, Wettwer E, Kortner A, Knaut M, Schuler S, Ravens U. Human inward rectifier potassium channels in chronic and postoperative atrial fibrillation. Cardiovasc Res. 2002;54:397–404. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
