

Adverse outcomes in surgical patients: implementation of a nationwide reporting system
- PMID: 17074866
- PMCID: PMC2565813
- DOI: 10.1136/qshc.2005.016220
Adverse outcomes in surgical patients: implementation of a nationwide reporting system
Abstract
Problem: Lack of comparable data on adverse outcomes in hospitalised surgical patients.
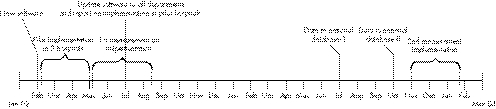
Design: A Plan-Do-Study-Act (PDSA) cycle to implement and evaluate nationwide uniform reporting of adverse outcomes in surgical patients. Evaluation was done within the Reach Efficacy-Adoption Implementation Maintenance (RE-AIM) framework.
Setting: All 109 surgical departments in The Netherlands.
Key measures for improvement: Increase in the number of departments implementing the reporting system and exporting data to the national database.
Strategies for change: The intervention included (1) a coordinator who could mediate in case of problems; (2) participation of an opinion leader; (3) a predefined plan of action communicated to all departments (including feedback of results during implementation); (4) connection with existing hospital databases; (5) provision of software and a helpdesk; and (6) an instrument based on nationwide standards.
Effects of change: Implementation increased from 18% to 34% in 1.5 years. The main reason for not implementing the system was that the Information Computer Technology (ICT) department did not link data with the hospital information system (lack of time, finances, low priority). Only 5% of the departments exported data to the national database. Export of data was hindered mainly by slow implementation of the reporting system (so that departments did not have data to export) and by concerns regarding data quality and public availability of data from individual hospitals.
Lessons learned: Hospitals need incentives to realise implementation. Important factors are financial support, sufficient manpower, adequate ICT linkage of data, and clarity with respect to public availability of data.
Conflict of interest statement
Conflict of interest: none.
References
-
- Marang‐van de Mheen P J, Kievit J. Automated registration of adverse events in surgical patients in the Netherlands: the current status (in Dutch). Ned Tijdschr Geneeskd 20031471273–1277. - PubMed
-
- Brennan T A, Leape L L, Laird N M.et al Incidence of adverse outcomes and negligence in hospitalized patients: results of the Havard Medical Practice Study I. N Engl J Med 1991324370–376. - PubMed
-
- Gawande A A, Thomas E J, Zinner M J.et al The incidence and nature of surgical adverse outcomes in Colorado and Utah in 1992. Surgery 199912666–75. - PubMed
-
- Kable A K, Gibberd R W, Spigelman A D. Adverse outcomes in surgical patients in Australia. Int J Qual Health Care 200214269–276. - PubMed
-
- Davis P, Ley‐Yee R, Briant R.et alAdverse outcomes in New Zealand Public Hospitals: principal findings from a national survey. Occasional Paper No 3. New Zealand: Ministry of Health, 2001
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical