

Reduced morbidity for elderly patients with a hip fracture after implementation of a perioperative evidence-based clinical pathway
- PMID: 17074877
- PMCID: PMC2565826
- DOI: 10.1136/qshc.2005.017095
Reduced morbidity for elderly patients with a hip fracture after implementation of a perioperative evidence-based clinical pathway
Abstract
Background: Hip fractures, common in the elderly population, result in significant morbidity and mortality. A study was undertaken to determine how an evidence based clinical pathway (CP) for treatment of elderly patients with hip fracture affected morbidity, in-hospital mortality, and health service utilization.
Methods: A pre-post study design using two population based inception cohorts of hip fracture patients aged > or =65 years was used. The control group (n = 678) was enrolled between July 1996 and September 1997 before implementation of the pathway and the CP group (n = 663) was enrolled between July 1999 and September 2000 following pathway implementation. Chart reviews were completed during study time frames to determine complications, mortality, and health service utilization.
Results: Only nine patients (1%) in the CP group experienced postoperative congestive heart failure compared with 37 (5%) control patients (p<0.001). Postoperative cardiac arrythmias were significantly lower in the CP group than in the control group (8 (1%) v 36 (5%); p<0.001). Postoperative delirium occurred in 22% of the CP group and 51% of the control group (p<0.001). There was no difference in risk adjusted in-hospital mortality between the two groups. Overall length of stay (LOS) and costs were unchanged between the groups; however, hospital LOS increased while rehabilitation LOS decreased in the CP group.
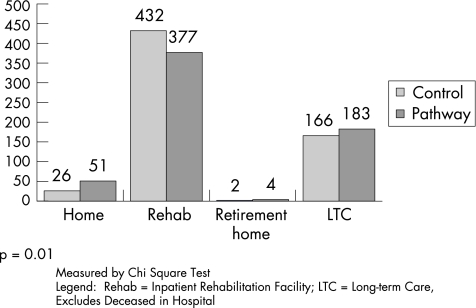
Conclusion: Implementation of an evidence based clinical pathway reduced postoperative morbidity and did not affect in-hospital mortality or overall costs of inpatient care. The effect of changing trends in medical care cannot be ruled out, but the reduction in complications in several clinical areas lends support to the positive impact of the clinical pathway. Perioperative CP is one successful management approach for this fragile patient population as patient morbidity was reduced without negatively affecting resource utilization.
Conflict of interest statement
Competing interests: none.
References
-
- Brainsky A, Glick H, Lydick E.et al The economic cost of hip fractures in community‐dwelling older adults: a prospective study. J Am Geriatr Soc 199745281–287. - PubMed
-
- Johnell O, Kanis J. Epidemiology of osteoporotic fractures. Osteoporos Int 200516S3–S7. - PubMed
-
- Donald I P, Bulpitt C J. The prognosis of falls in elderly people living at home. Age Ageing 199928121–125. - PubMed
-
- Wiktorowicz M E, Goeree R, Papaioannou A.et al Economic implications of hip fracture: health service use, institutional care and cost in Canada. Osteopor Int 200112271–278. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous