

Late-onset acute rejection after living donor liver transplantation
- PMID: 17075982
- PMCID: PMC4125674
- DOI: 10.3748/wjg.v12.i41.6674
Late-onset acute rejection after living donor liver transplantation
Abstract
Aim: To investigate the incidence and risk factors of late-onset acute rejection (LAR) and to clarify the effectiveness of our immunosuppressive regime consisting of life-long administration of tacrolimus and steroids.
Methods: Adult living donor liver transplantation recipients (n=204) who survived more than 6 mo after living donor liver transplantation were enrolled. Immunosuppression was achieved using tacrolimus and methylprednisolone. When adverse effects of tacrolimus were detected, the patient was switched to cyclosporine. Six months after transplantation, tacrolimus or cyclosporine was carefully maintained at a therapeutic level. The methylprednisolone dosage was maintained at 0.05 mg/kg per day by oral administration. Acute rejections that occurred more than 6 mo after the operation were defined as late-onset. The median follow-up period was 34 mo.
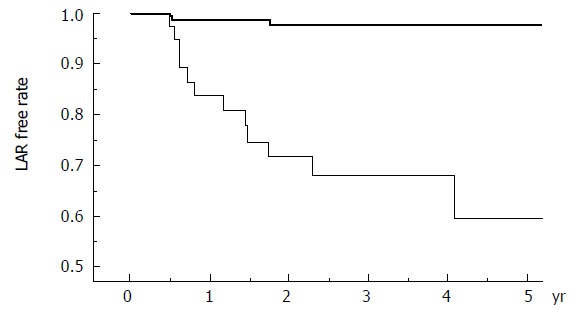
Results: LAR was observed in 15 cases (7%) and no chronic rejection was observed. The incidence of hyperlipidemia, chronic renal failure, new-onset post-transplantation diabetes, and deep fungal infection were 13%, 2%, 24%, and 17%, respectively. Conversion from tacrolimus to cyclosporine was required in 38 patients (19%). Multivariate analysis revealed that a cyclosporine-based regimen was significantly associated with LAR.
Conclusion: Both LAR and drug-induced adverse events happen at a low incidence, supporting the safety and efficacy of the present immunosuppression regimen for living donor liver transplantation.
Figures
References
-
- Busuttil RW, Lake JR. Role of tacrolimus in the evolution of liver transplantation. Transplantation. 2004;77:S44–S51. - PubMed
-
- Greig P, Lilly L, Scudamore C, Erb S, Yoshida E, Kneteman N, Bain V, Ghent C, Marotta P, Grant D, et al. Early steroid withdrawal after liver transplantation: the Canadian tacrolimus versus microemulsion cyclosporin A trial: 1-year follow-up. Liver Transpl. 2003;9:587–595. - PubMed
-
- Pirenne J, Aerts R, Koshiba T, Van Gelder F, Roskams T, Schetz M, Verhaegen M, Lauwers P, Fevery J, Nevens F. Steroid-free immunosuppression during and after liver transplantation--a 3-yr follow-up report. Clin Transplant. 2003;17:177–182. - PubMed
-
- Pageaux GP, Calmus Y, Boillot O, Ducerf C, Vanlemmens C, Boudjema K, Samuel D. Steroid withdrawal at day 14 after liver transplantation: a double-blind, placebo-controlled study. Liver Transpl. 2004;10:1454–1460. - PubMed
-
- Boillot O, Mayer DA, Boudjema K, Salizzoni M, Gridelli B, Filipponi F, Trunecka P, Krawczyk M, Clavien PA, Ducerf C, et al. Corticosteroid-free immunosuppression with tacrolimus following induction with daclizumab: a large randomized clinical study. Liver Transpl. 2005;11:61–67. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
