

Helicobacter cinaedi cellulitis and bacteremia in immunocompetent hosts after orthopedic surgery
- PMID: 17079500
- PMCID: PMC1828951
- DOI: 10.1128/JCM.01507-06
Helicobacter cinaedi cellulitis and bacteremia in immunocompetent hosts after orthopedic surgery
Abstract
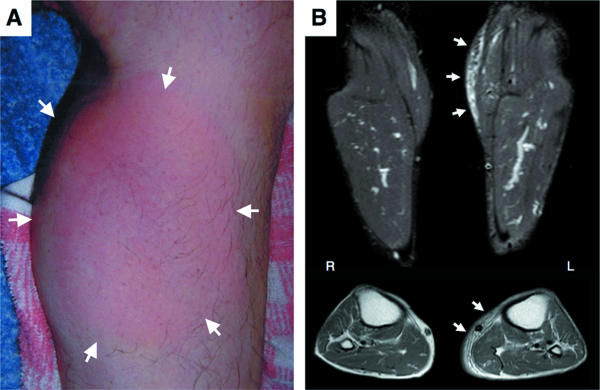
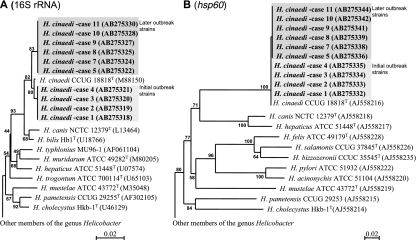
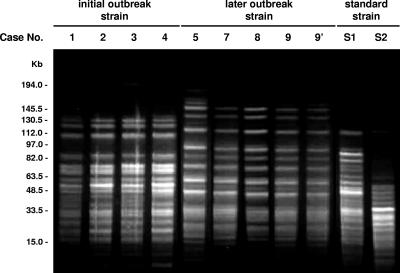
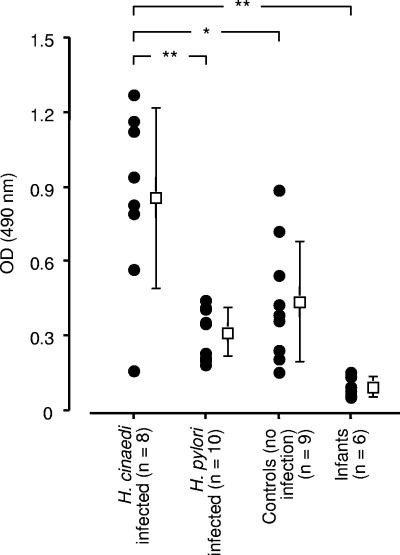
At various times after orthopedic operations (more than a few weeks, with an average of 29.9 days), 11 patients had a sudden onset of high temperature (average 38.9 degrees C) and local cellulitis at different sites on the operated sides. The wounds had completely healed, without complicated infections, when the cellulitis occurred. The clinical picture of cellulitis in all patients was atypical: diffuse salmon-pink skin color, local heat, swelling, spontaneous pain, and tenderness but no eruptions. No patient had any underlying immunocompromising conditions or had been given immunosuppressive agents. Gram-negative spiral bacteria were isolated from blood cultures and were identified as Helicobacter cinaedi on the basis of 16S rRNA gene sequencing and DNA-DNA hybridization using standard strains. By means of phylogenetic analysis, we divided these clinical isolates into two clones. The H. cinaedi strain isolated via fecal cultures from two patients without intestinal symptoms was the same clone as the blood isolate. All isolates were quite susceptible to various antibiotics, and clinical and inflammatory symptoms of bacteremia and cellulitis improved after treatment with penicillins and cephalosporins. A relatively high incidence of recurrence of the same disease was observed, however. Almost all patients responded immunologically to the infection, as evidenced by the production of serum antibody against H. cinaedi. We thus suggest that H. cinaedi should not be regarded as simply an opportunistic pathogen but that it may be a pathogen in immunocompetent hosts and may cause infections together with bacteremia and cellulitis.
Figures

References
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
