

Causes of death and determinants of outcome in critically ill patients
- PMID: 17083735
- PMCID: PMC1794454
- DOI: 10.1186/cc5086
Causes of death and determinants of outcome in critically ill patients
Abstract
Introduction: Whereas most studies focus on laboratory and clinical research, little is known about the causes of death and risk factors for death in critically ill patients.
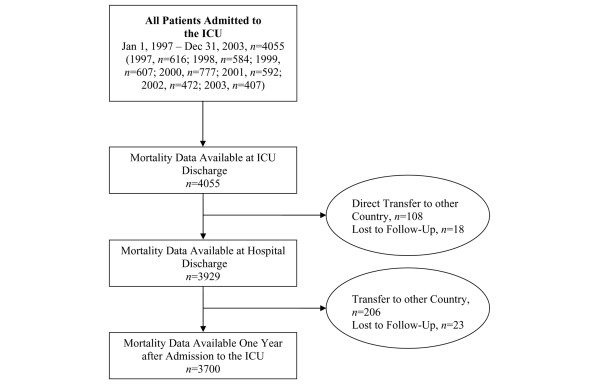
Methods: Three thousand seven hundred patients admitted to an adult intensive care unit (ICU) were prospectively evaluated. Study endpoints were to evaluate causes of death and risk factors for death in the ICU, in the hospital after discharge from ICU, and within one year after ICU admission. Causes of death in the ICU were defined according to standard ICU practice, whereas deaths in the hospital and at one year were defined and grouped according to the ICD-10 (International Statistical Classification of Diseases and Related Health Problems) score. Stepwise logistic regression analyses were separately calculated to identify independent risk factors for death during the given time periods.
Results: Acute, refractory multiple organ dysfunction syndrome was the most frequent cause of death in the ICU (47%), and central nervous system failure (relative risk [RR] 16.07, 95% confidence interval [CI] 8.3 to 31.4, p < 0.001) and cardiovascular failure (RR 11.83, 95% CI 5.2 to 27.1, p < 0.001) were the two most important risk factors for death in the ICU. Malignant tumour disease and exacerbation of chronic cardiovascular disease were the most frequent causes of death in the hospital (31.3% and 19.4%, respectively) and at one year (33.2% and 16.1%, respectively).
Conclusion: In this primarily surgical critically ill patient population, acute or chronic multiple organ dysfunction syndrome prevailed over single-organ failure or unexpected cardiac arrest as a cause of death in the ICU. Malignant tumour disease and chronic cardiovascular disease were the most important causes of death after ICU discharge.
Figures
References
-
- Knaus WA, Wagner DP, Zimmerman JE, Draper EA. Variations in mortality and length of stay in intensive care units. Ann Intern Med. 1993;118:753–761. - PubMed
-
- Benoit DD, Vandewoude KH, Decruyenaere JM, Hoste EA, Colardyn FA. Outcome and early prognostic indicators in patients with a hematologic malignancy admitted to the intensive care unit for a life-threatening complication. Crit Care Med. 2003;31:104–112. doi: 10.1097/00003246-200301000-00017. - DOI - PubMed
-
- Afessa B, Morales IJ, Scanlon PD, Peters SG. Prognostic factors, clinical course, and hospital outcome of patients with chronic obstructive pulmonary disease admitted to an intensive care unit for acute respiratory failure. Crit Care Med. 2002;30:1610–1615. doi: 10.1097/00003246-200207000-00035. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
