

Early onset of selective serotonin reuptake inhibitor antidepressant action: systematic review and meta-analysis
- PMID: 17088502
- PMCID: PMC2211759
- DOI: 10.1001/archpsyc.63.11.1217
Early onset of selective serotonin reuptake inhibitor antidepressant action: systematic review and meta-analysis
Abstract
Context: Selective serotonin reuptake inhibitors (SSRIs) are often described as having a delayed onset of effect in the treatment of depression. However, some trials have reported clinical improvement as early as the first week of treatment.
Objective: To test the alternative hypotheses of delayed vs early onset of antidepressant action with SSRIs in patients with unipolar depression.
Data sources: Trials identified by searching CENTRAL, The Cochrane Collaboration database of controlled trials (2005), and the reference lists of identified trials and other systematic reviews.
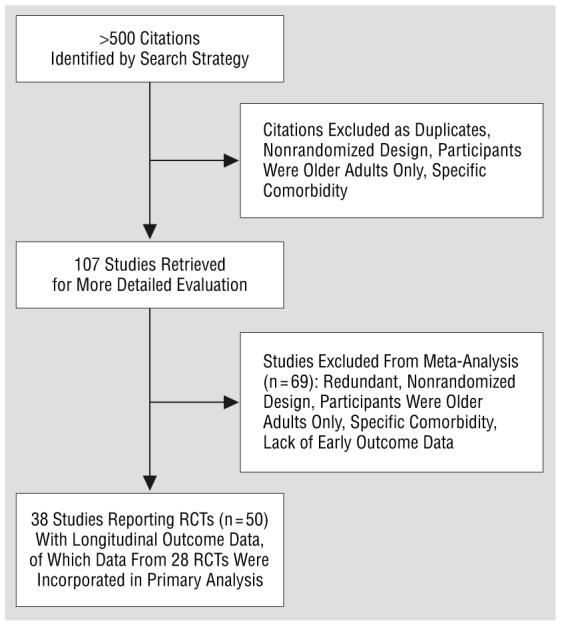
Study selection: Randomized controlled trials of SSRIs vs placebo for the treatment of unipolar depression in adults that reported outcomes for at least 2 time points in the first 4 weeks of treatment (50 trials from >500 citations identified). Trials were excluded if limited to participants older than 65 years or specific comorbidities.
Data extraction: Data were extracted on trial design, participant characteristics, and outcomes by a single reviewer.
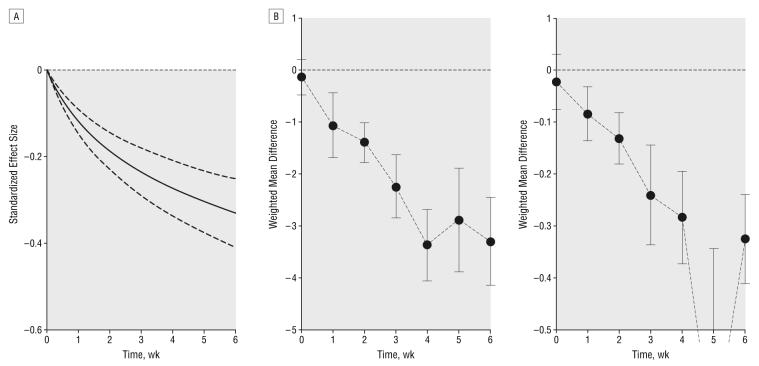
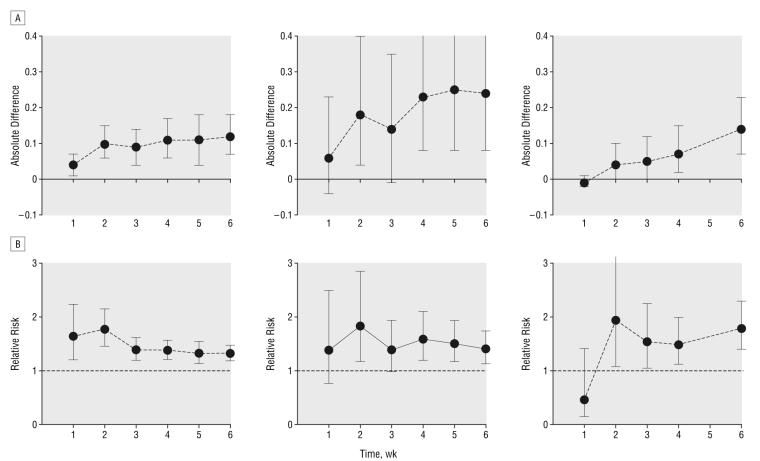
Data synthesis: Pooled estimates of treatment effect on depressive symptom rating scales were calculated for weeks 1 through 6 of treatment. In the primary analysis, the pattern of response seen was tested against alternative models of onset of response. The primary analysis incorporated data from 28 randomized controlled trials (n=5872). A model of early treatment response best fit the experimental data. Treatment with SSRIs rather than placebo was associated with clinical improvement by the end of the first week of use. A secondary analysis indicated an increased chance of achieving a 50% reduction in Hamilton Depression Rating Scale scores by 1 week (relative risk, 1.64; 95% confidence interval, 1.2-2.25) with SSRI treatment compared with placebo.
Conclusions: Treatment with SSRIs is associated with symptomatic improvement in depression by the end of the first week of use, and the improvement continues at a decreasing rate for at least 6 weeks.
Figures
Comment in
-
Review: SSRIs lead to improvement in depression by the end of the first week.Evid Based Med. 2007 Jun;12(3):72. doi: 10.1136/ebm.12.3.72. Evid Based Med. 2007. PMID: 17537880 No abstract available.
-
Publication bias in systematic reviews.Arch Gen Psychiatry. 2007 Jul;64(7):868. doi: 10.1001/archpsyc.64.7.868-a. Arch Gen Psychiatry. 2007. PMID: 17606823 No abstract available.
-
Review: response to SSRIs in unipolar depression occurs in the first week of treatment.Evid Based Ment Health. 2007 Aug;10(3):81. doi: 10.1136/ebmh.10.3.81. Evid Based Ment Health. 2007. PMID: 17652563 No abstract available.
References
-
- National Collaborating Centre for Mental Health . Depression: Management of Depression in Primary and Secondary Care. London, England: National Institute for Clinical Excellence; 2004. (Clinical Guideline 23).
-
- Blier P, de Montigny C. Current advances and trends in the treatment of depression. Trends Pharmacol Sci. 1994;15:220–226. - PubMed
-
- Duman RS. Depression: a case of neuronal life and death? Biol Psychiatry. 2004;56:140–145. - PubMed
-
- Banerjee SP, Kung LS, Riggi SJ, Chanda SK. Development of β-adrenergic receptor subsensitivity by antidepressants. Nature. 1977;268:455–456. - PubMed
-
- Quitkin FM, Rabkin JD, Markowitz JM, Stewart JW, McGrath PJ, Harrison W. Use of pattern analysis to identify true drug response: a replication. Arch Gen Psychiatry. 1987;44:259–264. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
