

In vitro evaluation of the air separation ability of four cardiovascular manufacturer extracorporeal circuit designs
- PMID: 17089505
- PMCID: PMC4680810
In vitro evaluation of the air separation ability of four cardiovascular manufacturer extracorporeal circuit designs
Abstract
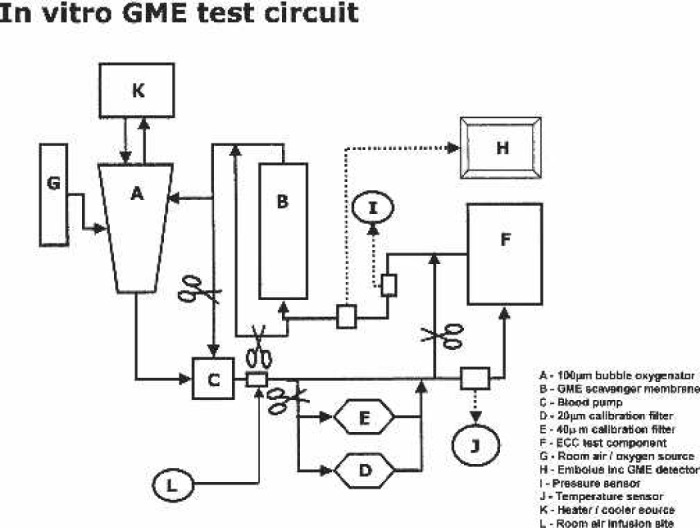
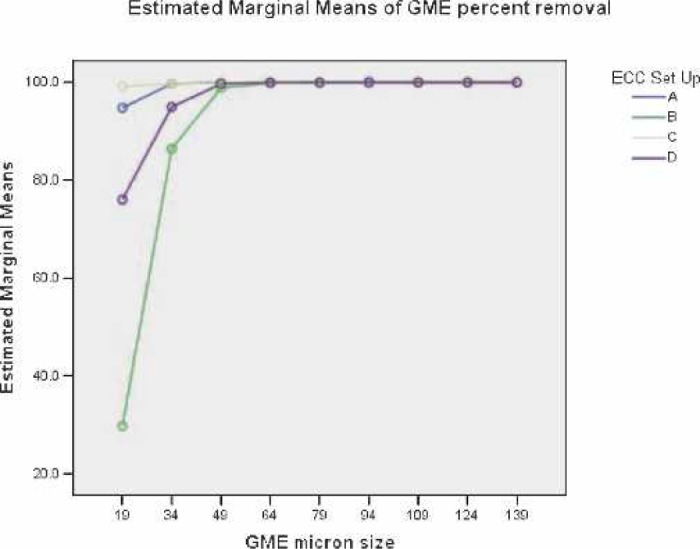
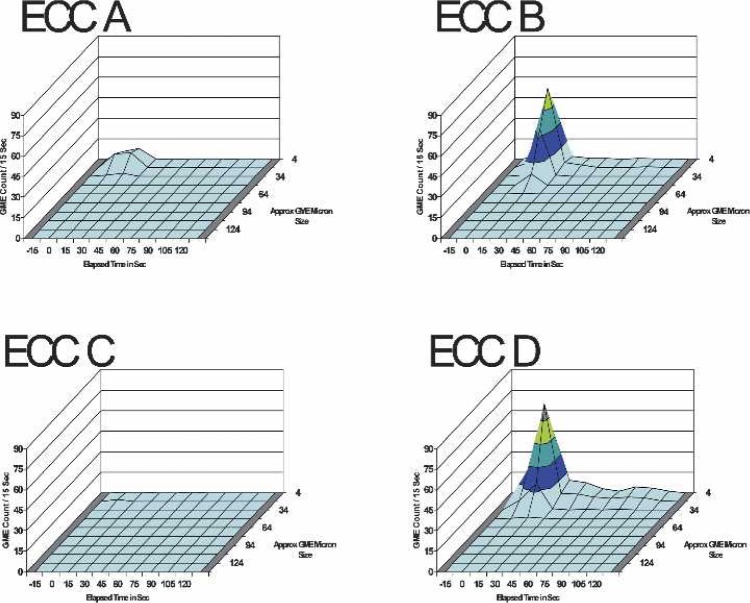
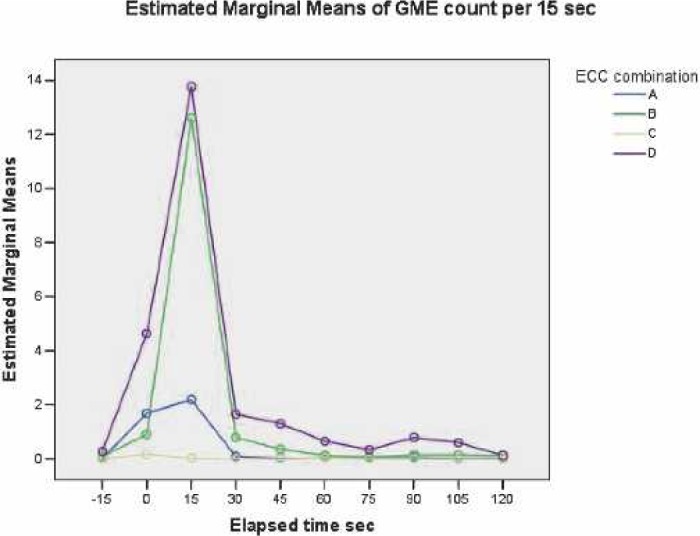
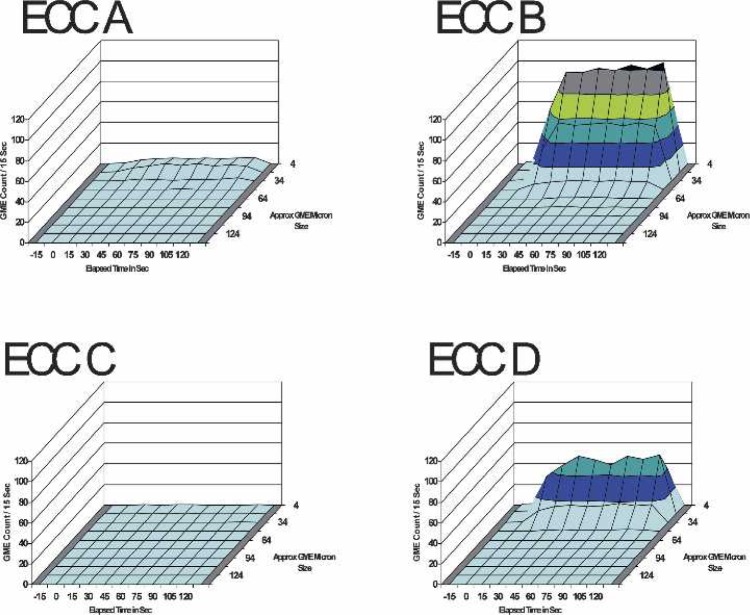
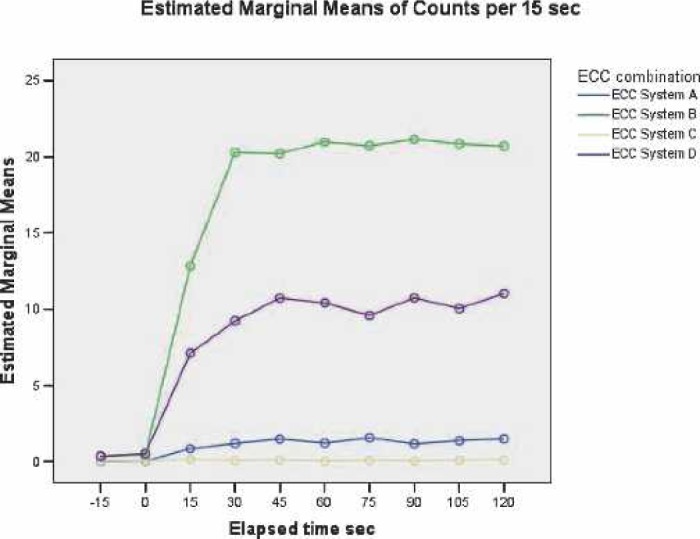
Neurologic impairment is a common complication of adult cardiac surgery. Cerebral gaseous microemboli (GME) detected during cardiopulmonary bypass has been associated with cognitive impairment after adult cardiac surgery. Several previous studies have shown that components comprising the extracorporeal circuit (ECC) can affect the ability of the ECC to eliminate air. The differences in the air separation ability of four manufacturer's commonly used ECCs were studied. The air-separating ability of Cobe Cardiovascular, Gish Biomedical, Medtronic, and Terumo Cardiovascular Systems Corp. ECCs were studied in vitro under clinically relevant conditions. Bolus and continuous venous air were introduced and output GME patterns by size, time, and count were measured (using an embolus detection device) and statistically analyzed. Graphic representations depicting elapsed time, GME size, and bubble count helped to visually rank the air-handling performance of the ECCs. There are significant air-handling differences between the ECCs tested. Overall, the blinded results reveal that ECC A and ECC C removed significantly (p < 0.001) more suspended GME than ECC B and ECC D. In the 50-mL venous room-air bolus and the 100 mL/min pulsed air challenges, ECC B and ECC D allowed significantly more GME to pass (p < 0.001) compared with ECC A and ECC C. For example, in a 2-hour pump run ECC C would deliver 480 potential high-intensity transient signals (HITS) compared with the 9600 from the ECC B during venous room air entrainment at 100 mL/min. There are substantial and significant air-handling differences between the ECCs from the four different manufacturers. The results from this work allow for objective characterization of ECCs air-separating ability. This additional information provides an opportunity for clinicians to potentially minimize the risks of arterial air embolization and its associated deleterious neurologic effects, while allowing clinicians to make better-informed consumer decisions.
Figures
Comment in
-
Normalization of deviance: rocket science 101.J Extra Corpor Technol. 2006 Sep;38(3):201-2. J Extra Corpor Technol. 2006. PMID: 17089504 Free PMC article. No abstract available.
-
Gaseous microemboli and hyperoxia.J Extra Corpor Technol. 2006 Dec;38(4):367-9. J Extra Corpor Technol. 2006. PMID: 17312918 Free PMC article. No abstract available.
-
In vitro evaluation of the air separation ability of four cardiovascular manufacturer extracorporeal circuit designs.J Extra Corpor Technol. 2007 Mar;39(1):55; author reply 55. J Extra Corpor Technol. 2007. PMID: 17486876 Free PMC article. No abstract available.
References
-
- Wong BI, McLean RF, Naylor CD, et al. Central nervous system dysfunction after warm or hypothermic cardiopulmonary bypass. Lancet. 1992;339:I383–4. - PubMed
-
- Shaw PJ, Bates D, Cartlidge NE, et al. Neurologic and neuropsychological morbidity following major surgery. Comparison of coronary artery bypass and peripheral vascular surgery. Stroke. 1987;18:700–7. - PubMed
-
- Roach GW, Kanchuger M, Mora M, et al. Adverse cerebral outcomes after coronary bypass surgery. N Engl J Med. 1996;335:1857–63. - PubMed
-
- Pugsley W, Klinger L, Paschalis C, et al. Microemboli and cerebral impairment during cardiac surgery. Vasc Surg. 1990;24:34–43.
MeSH terms
LinkOut - more resources
Full Text Sources