

Normoxia vs. hyperoxia: impact of oxygen tension strategies on outcomes for patients receiving cardiopulmonary bypass for routine cardiac surgical repair
- PMID: 17089511
- PMCID: PMC4680816
Normoxia vs. hyperoxia: impact of oxygen tension strategies on outcomes for patients receiving cardiopulmonary bypass for routine cardiac surgical repair
Abstract
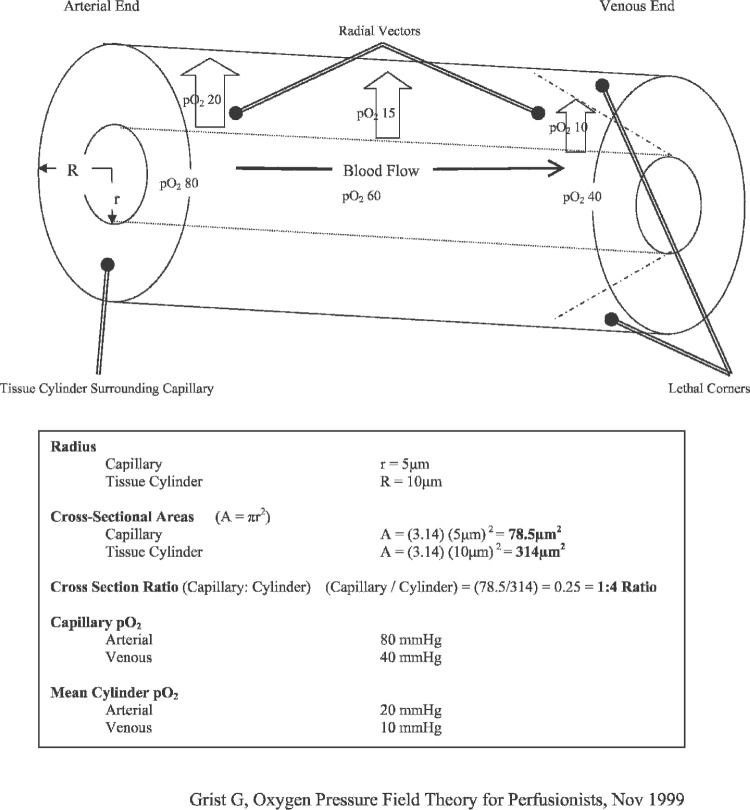
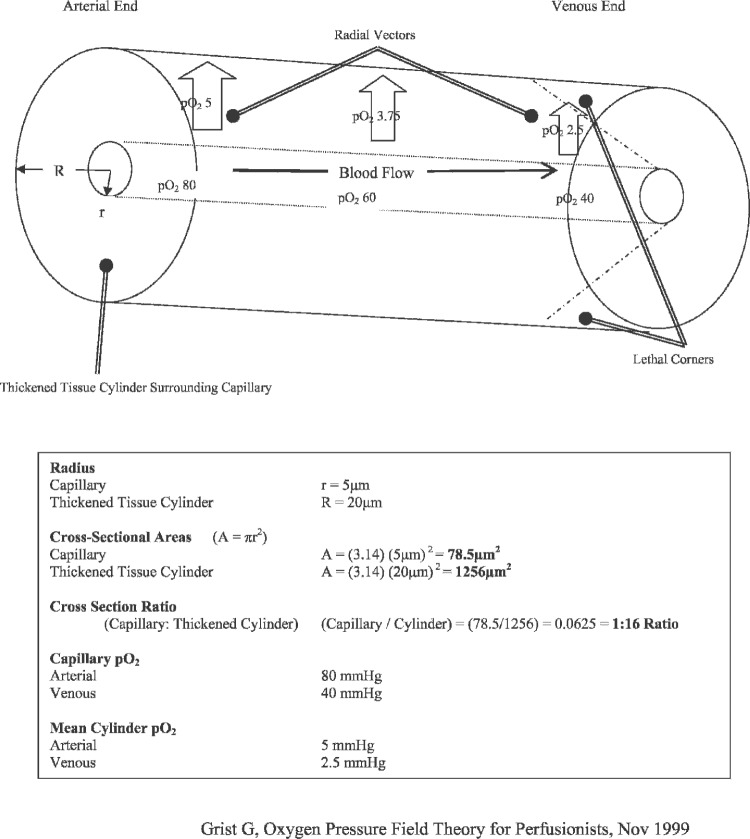
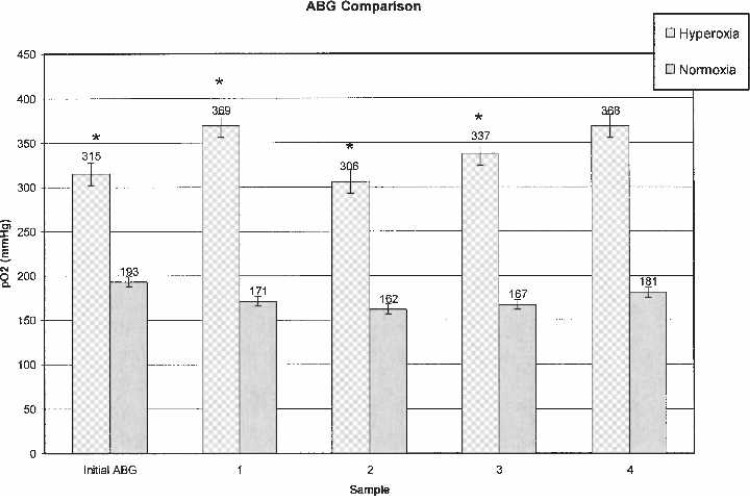
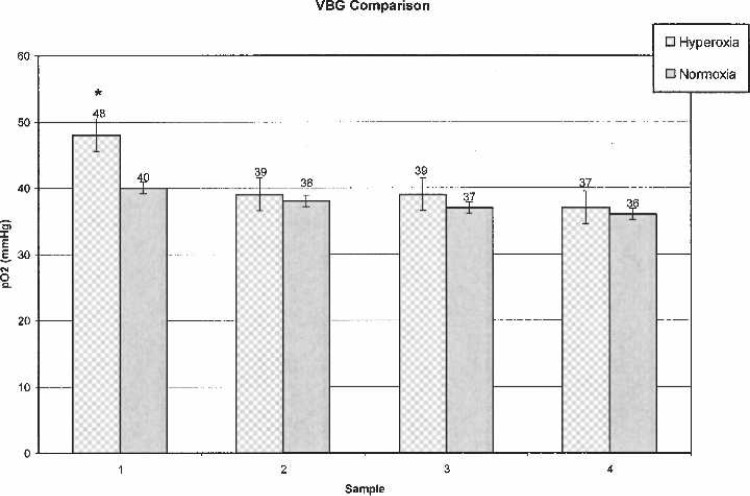
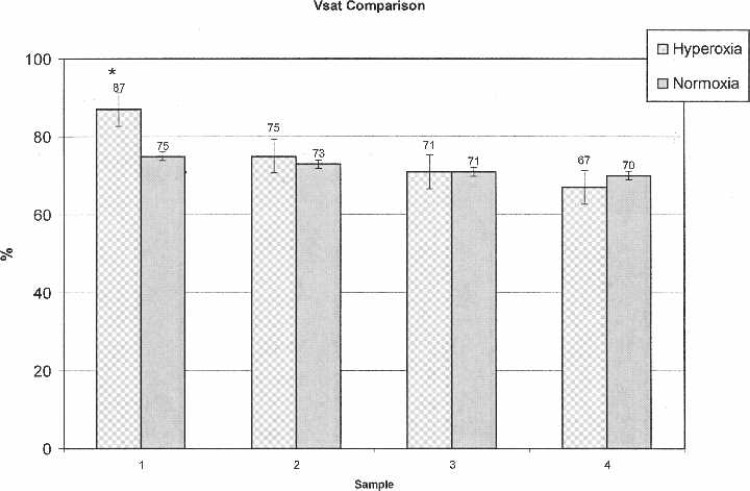
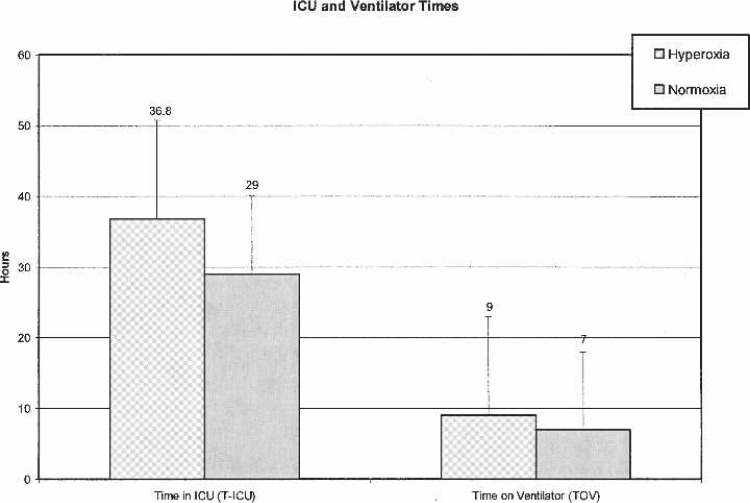
Oxygen pressure field theory (OPFT) was originally described in the early 1900s by Danish physiologist, Dr. August Krogh. This revolutionary theory described microcirculation of blood gases at the capillary level using a theoretical cylindrical tissue model commonly referred to as the Krogh cylinder. In recent years, the principles and benefits of OPFT in long-term extracorporeal circulatory support (ECMO) have been realized. Cardiac clinicians have successfully mastered OPFT fundamentals and incorporated them into their clinical practice. These clinicians have experienced significantly improved survival rates as a result of OPFT strategies. The objective of this study was to determine if a hyperoxic strategy can lead to equally beneficial outcomes for short-term support as measured by total ventilator time and total length of stay in intensive care unit (ICU) in the cardiopulmonary bypass (CPB) patient at a private institution. Patients receiving traditional blood gas management while on CPB (group B, n = 17) were retrospectively compared with hyperoxic patients (group A, n = 19). Hyperoxic/OPFT management was defined as paO2 values of 300-350 mmHg and average VSAT > 75%. Traditional blood gas management was defined as paO2 values of 150-250 mmHg and average VSAT < 75%. No significant differences between treatment groups were found for patient weight, CPB/AXC times, BSA, pre/post Hgb, pre/post-platelet (PLT) counts, pre/post-creatinine levels, pre/ post-BUN, UF volumes, or CPB urine output. Additionally, no significant statistical differences were found between treatment groups for total time in ICU (T-ICU) or total time on ventilator (TOV). Hyperoxic management strategies provided no conclusive evidence of outcome improvement for patients receiving CPB for routine cardiac surgical repair. Additional studies into the impact of hyperoxia in short-term extracorporeal circulatory support are needed.
Conflict of interest statement
The senior author has stated that authors have reported no material, financial or other relationship with any healthcare-related business or other entity whose products or services are discussed in this paper.
Figures
References
-
- Grist G, Thomas D.. Blood anion gaps and venoarterial carbon dioxide gradients as risk factors in long-term extracorporeal support. J Extra Corpor Technol. 1997;29:6–10. - PubMed
-
- Gutierrez G, Lund N, Bryan-Brown CW.. Cellular oxygen during multiple organ failure. Crit Care Clin. 1989;5:271–87. - PubMed
-
- Sharan M, Gupta S, Popel AS.. Parametric analysis of the relationship between end-capillary and mean tissue pO2 as predicted by a mathematical model. J Theor Biol. 1998;195:439–49. - PubMed
-
- Schumacker PT, Samsel RW.. Analysis of oxygen delivery and re-uptake relationships in the Krogh tissue model. J Appl Physiol. 1989;67:1234–44. - PubMed
-
- Walfridsson H, Lund N.. Tissue oxygen pressure in normal myocardium and across the border zone during coronary artery occlusion in the pig. Effects of different arterial oxygen pressures. Basic Res Cardiol. 1990;85:467–80. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical