

Angiotensin II causes hypertension and cardiac hypertrophy through its receptors in the kidney
- PMID: 17090678
- PMCID: PMC1693859
- DOI: 10.1073/pnas.0605545103
Angiotensin II causes hypertension and cardiac hypertrophy through its receptors in the kidney
Abstract
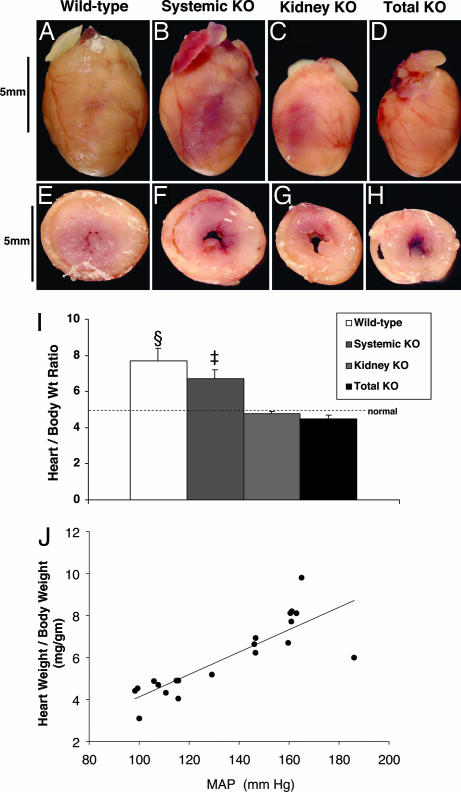
Essential hypertension is a common disease, yet its pathogenesis is not well understood. Altered control of sodium excretion in the kidney may be a key causative feature, but this has been difficult to test experimentally, and recent studies have challenged this hypothesis. Based on the critical role of the renin-angiotensin system (RAS) and the type I (AT1) angiotensin receptor in essential hypertension, we developed an experimental model to separate AT1 receptor pools in the kidney from those in all other tissues. Although actions of the RAS in a variety of target organs have the potential to promote high blood pressure and end-organ damage, we show here that angiotensin II causes hypertension primarily through effects on AT1 receptors in the kidney. We find that renal AT1 receptors are absolutely required for the development of angiotensin II-dependent hypertension and cardiac hypertrophy. When AT1 receptors are eliminated from the kidney, the residual repertoire of systemic, extrarenal AT1 receptors is not sufficient to induce hypertension or cardiac hypertrophy. Our findings demonstrate the critical role of the kidney in the pathogenesis of hypertension and its cardiovascular complications. Further, they suggest that the major mechanism of action of RAS inhibitors in hypertension is attenuation of angiotensin II effects in the kidney.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, et al. Hypertension. 2003;42:1206–1252. - PubMed
-
- Guyton AC. Science. 1991;252:1813–1816. - PubMed
-
- Lifton RP, Gharavi AG, Geller DS. Cell. 2001;104:545–556. - PubMed
-
- Brenner R, Perez GJ, Bonev AD, Eckman DM, Kosek JC, Wiler SW, Patterson AJ, Nelson MT, Aldrich RW. Nature. 2000;407:870–876. - PubMed
-
- Zhu Y, Bian Z, Lu P, Karas RH, Bao L, Cox D, Hodgin J, Shaul PW, Thoren P, Smithies O, et al. Science. 2002;295:505–508. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
