

Multicentre study on peri- and postoperative central venous oxygen saturation in high-risk surgical patients
- PMID: 17101038
- PMCID: PMC1794462
- DOI: 10.1186/cc5094
Multicentre study on peri- and postoperative central venous oxygen saturation in high-risk surgical patients
Abstract
Introduction: Low central venous oxygen saturation (ScvO2) has been associated with increased risk of postoperative complications in high-risk surgery. Whether this association is centre-specific or more generalisable is not known. The aim of this study was to assess the association between peri- and postoperative ScvO2 and outcome in high-risk surgical patients in a multicentre setting.
Methods: Three large European university hospitals (two in Finland, one in Switzerland) participated. In 60 patients with intra-abdominal surgery lasting more than 90 minutes, the presence of at least two of Shoemaker's criteria, and ASA (American Society of Anesthesiologists) class greater than 2, ScvO2 was determined preoperatively and at two hour intervals during the operation until 12 hours postoperatively. Hospital length of stay (LOS) mortality, and predefined postoperative complications were recorded.
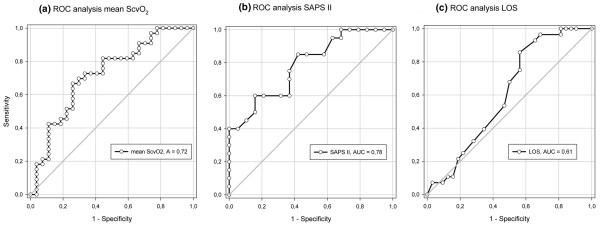
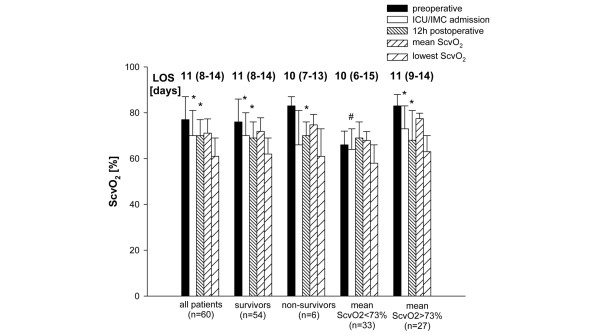
Results: The age of the patients was 72 +/- 10 years (mean +/- standard deviation), and simplified acute physiology score (SAPS II) was 32 +/- 12. Hospital LOS was 10.5 (8 to 14) days, and 28-day hospital mortality was 10.0%. Preoperative ScvO2 decreased from 77% +/- 10% to 70% +/- 11% (p < 0.001) immediately after surgery and remained unchanged 12 hours later. A total of 67 postoperative complications were recorded in 32 patients. After multivariate analysis, mean ScvO2 value (odds ratio [OR] 1.23 [95% confidence interval (CI) 1.01 to 1.50], p = 0.037), hospital LOS (OR 0.75 [95% CI 0.59 to 0.94], p = 0.012), and SAPS II (OR 0.90 [95% CI 0.82 to 0.99], p = 0.029) were independently associated with postoperative complications. The optimal value of mean ScvO2 to discriminate between patients who did or did not develop complications was 73% (sensitivity 72%, specificity 61%).
Conclusion: Low ScvO2 perioperatively is related to increased risk of postoperative complications in high-risk surgery. This warrants trials with goal-directed therapy using ScvO2 as a target in high-risk surgery patients.
Figures

Comment in
-
Should we use central venous saturation to guide management in high-risk surgical patients?Crit Care. 2006;10(6):181. doi: 10.1186/cc5122. Crit Care. 2006. PMID: 17184557 Free PMC article.
References
-
- Shoemaker WC, Appel PL, Kram HB, Waxman K, Lee TS. Prospective trial of supranormal values of survivors as therapeutic goals in high-risk surgical patients. Chest. 1988;94:1176–1186. - PubMed
-
- Polonen P, Ruokonen E, Hippelainen M, Poyhonen M, Takala J. A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Anesth Analg. 2000;90:1052–1059. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
