

Transfer for urgent percutaneous coronary intervention early after thrombolysis for ST-elevation myocardial infarction: the TRANSFER-AMI pilot feasibility study
- PMID: 17102829
- PMCID: PMC2569051
- DOI: 10.1016/s0828-282x(06)70948-5
Transfer for urgent percutaneous coronary intervention early after thrombolysis for ST-elevation myocardial infarction: the TRANSFER-AMI pilot feasibility study
Abstract
Background: Most hospitals in Canada do not have percutaneous coronary intervention (PCI) facilities and use thrombolysis as reperfusion therapy for ST-elevation myocardial infarction (STEMI). Urgent PCI after thrombolysis may optimize reperfusion and prevent reinfarction and recurrent ischemia.
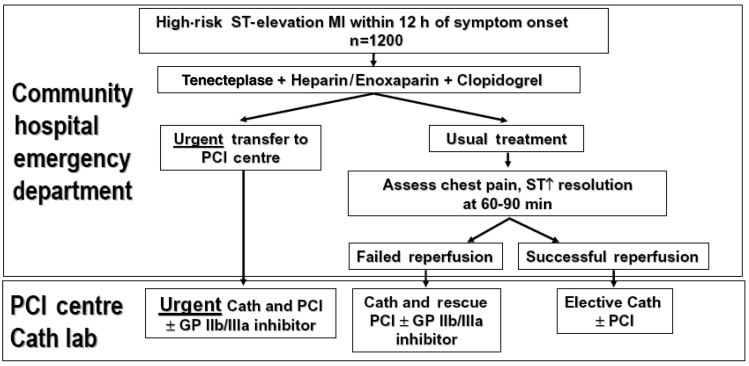
Objective: To determine the feasibility of transferring high-risk STEMI patients from community hospitals in Ontario to PCI centres for urgent PCI within 6 h of thrombolysis.
Methods: Patients with anterior or high-risk inferior STEMI received tenecteplase and were urgently transferred to PCI centres. PCI was performed if at least 70% stenosis was present in the infarct-related artery, regardless of flow, using coronary stents. Transfer of stable patients back to community hospitals was encouraged 24 h to 48 h after PCI.
Results: Eighteen patients were transferred and underwent PCI a median of 3.9 h (range 2.7 h to 6.4 h) after thrombolysis. No complications occurred during transfer. One death occurred that was related to failed reperfusion and cardiogenic shock. Minor access-site bleeding occurred in five patients. Fifteen patients were transferred back to their community hospitals within 24 h of PCI. There were no further deaths or reinfarctions at one-year follow-up.
Conclusions: Transfer of high-risk STEMI patients for urgent PCI within 6 h after thrombolysis appears feasible. The randomized trial phase of the Trial of Routine ANgioplasty and Stenting after Fibrinolysis to Enhance Reperfusion in Acute Myocardial Infarction (TRANSFER-AMI) will compare this strategy with standard treatment after thrombolysis.
HISTORIQUE: La plupart des hôpitaux du Canada ne possèdent pas d’installations pour effectuer des interventions coronaires percutanées (ICP) et utilisent la thrombolyse comme traitement de reperfusion en cas d’infarctus du myocarde avec surélévation du segment ST (IMSSST). Une ICP d’urgence après une thrombolyse peut optimiser la reperfusion et prévenir un nouvel infarctus et une ischémie récurrente.
OBJECTIF: Déterminer la faisabilité de transférer les patients atteints d’un IMSSST à haut risque des hôpitaux généraux ontariens vers des centres d’ICP pour subir une ICP d’urgence dans les six heures suivant une thrombolyse.
MÉTHODOLOGIE: Les patients atteints d’un IMSSST antérieur ou inférieur à haut risque ont reçu de la ténectéplase et ont été transférés d’urgence à un centre d’ICP. L’ICP était effectuée en cas de sténose d’au moins 70 % de l’artère infarcie, quel que soit le débit, au moyen d’une endoprothèse coronarienne. Le transfert des patients stables vers leur hôpital général était encouragé de 24 heures à 48 heures après l’ICP.
RÉSULTATS: Dix-huit patients ont été transférés et ont subi une ICP selon une médiane de 3,9 heures (fourchette de 2,7 heures à 6,4 heures) après une thrombolyse. Aucune complication ne s’est produite pendant le transfert. Un décès a eu lieu, relié à l’échec de la reperfusion et à un choc cardiogène. Cinq patients ont subi une hémorragie mineure au foyer d’accès. Quinze patients ont été transférés à leur hôpital général d’origine dans les 24 heures suivant l’ICP. Aucun autre décès ou infarctus n’avait eu lieu au suivi d’un an.
CONCLUSIONS: Le transfert des patients atteints d’un IMSSST à haut risque afin de subir une ICP d’urgence dans les six heures suivant une thrombolyse semble faisable. La phase d’essai aléatoire de l’essai TRANSFER-AMI sur l’angioplastie systématique et l’endoprothèse après une fibrinolyse pour améliorer la reperfusion en cas d’infarctus aigu du myocarde permettra de comparer cette stratégie au traitement standard après une thrombolyse.
Figures
References
-
- Armstrong PW, Bogaty P, Buller CE, Dorian P, O’Neill BJ. The 2004 ACC/AHA Guidelines: A perspective and adaptation for Canada by the Canadian Cardiovascular Society Working Group. Can J Cardiol. 2004;20:1075–9. - PubMed
-
- Cantor WJ, Ohman EM. ‘Facilitated’ PCI for acute MI: PCI with lysis and platelet inhibition. Curr Interv Cardiol Reports. 2001;3:321–9. - PubMed
-
- Antman EM, Anbe DT, Armstrong PW, et al. American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Canadian Cardiovascular Society. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (committee to revise the 1999 guidelines for the management of patients with acute myocardial infarction) Circulation. 2004;110:e82–292. - PubMed
-
- Bovill EG, Terrin ML, Stump DC, et al. Hemorrhagic events during therapy with recombinant tissue-type plasminogen activator, heparin, and aspirin for acute myocardial infarction. Results of the Thrombolysis in Myocardial Infarction (TIMI), Phase II Trial. Ann Intern Med. 1991;115:256–65. - PubMed
-
- An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. The GUSTO investigators. N Engl J Med. 1993;329:673–82. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
