

Randomized trial of percutaneous coronary intervention for subacute infarct-related coronary artery occlusion to achieve long-term patency and improve ventricular function: the Total Occlusion Study of Canada (TOSCA)-2 trial
- PMID: 17105848
- PMCID: PMC2785021
- DOI: 10.1161/CIRCULATIONAHA.106.669432
Randomized trial of percutaneous coronary intervention for subacute infarct-related coronary artery occlusion to achieve long-term patency and improve ventricular function: the Total Occlusion Study of Canada (TOSCA)-2 trial
Abstract
Background: In the present study, we sought to determine whether opening a persistently occluded infarct-related artery (IRA) by percutaneous coronary intervention (PCI) in patients beyond the acute phase of myocardial infarction (MI) improves patency and indices of left ventricular (LV) size and function.
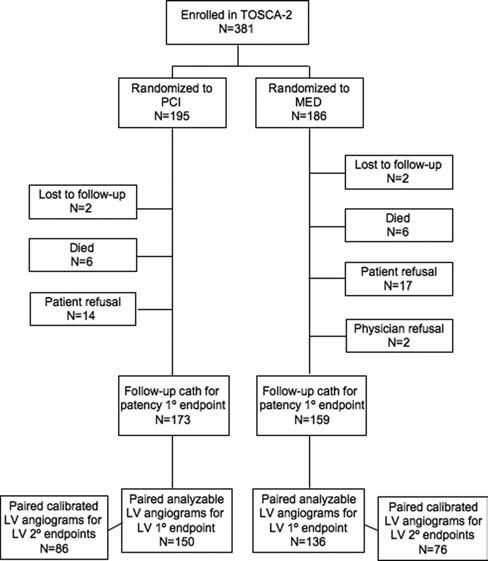
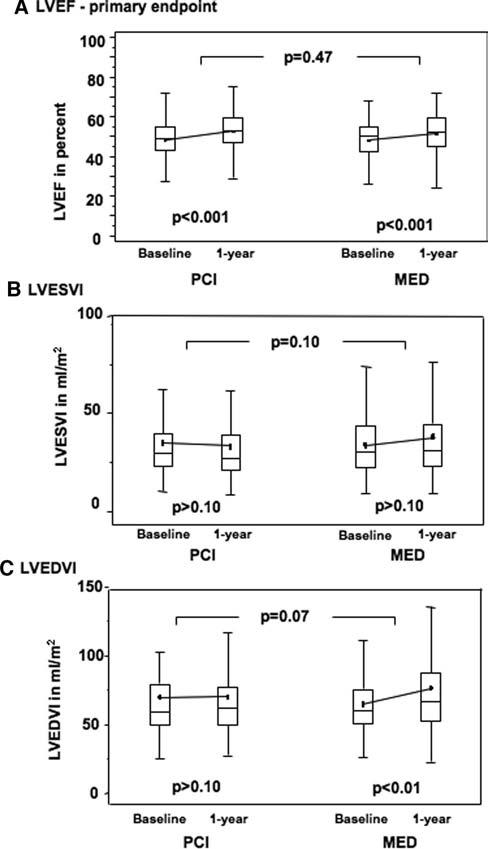
Methods and results: Between May 2000 and July 2005, 381 patients with an occluded native IRA 3 to 28 days after MI (median 10 days) were randomized to PCI with stenting (PCI) or optimal medical therapy alone. Repeat coronary and LV angiography was performed 1 year after randomization (n=332, 87%). Coprimary end points were IRA patency and change in LV ejection fraction. Secondary end points included change in LV end-systolic and end-diastolic volume indices and wall motion. PCI was successful in 92%. At 1 year, 83% of PCI versus 25% of medical therapy-only patients had a patent IRA (P<0.001). LV ejection fraction increased significantly (P<0.001) in both groups, with no between-group difference: PCI 4.2+/-8.9 (n=150) versus medical therapy 3.5+/-8.2 (n=136; P=0.47). Median change (interquartile range) in LV end-systolic volume index was -0.5 (-9.3 to 5.0) versus 1.0 (-5.7 to 7.3) mL/m2 (P=0.10), whereas median change (interquartile range) in LV end-diastolic volume index was 3.2 (-8.2 to 13.3) versus 5.3 (-4.6 to 23.2) mL/m2 (P=0.07) in the PCI (n=86) and medical therapy-only (n=76) groups, respectively.
Conclusions: PCI with stenting of a persistently occluded IRA in the subacute phase after MI effectively maintains long-term patency but has no effect on LV ejection fraction. On the basis of these findings and the lack of clinical benefit in the main Occluded Artery Trial, routine PCI is not recommended for stable patients with a persistently occluded IRA after MI.
Figures
Comment in
-
Does late PCI improve long-term arterial patency and LV function in patients with arterial occlusion after MI?Nat Clin Pract Cardiovasc Med. 2007 May;4(5):252-3. doi: 10.1038/ncpcardio0857. Epub 2007 Mar 20. Nat Clin Pract Cardiovasc Med. 2007. PMID: 17375051 No abstract available.
References
-
- White HD, Braunwald E. Applying the open artery theory: use of predictive survival markers. Eur Heart J. 1998;19:1132–1139. - PubMed
-
- Hochman JS, Choo H. Limitation of myocardial infarct expansion by reperfusion independent of myocardial salvage. Circulation. 1987;75:299–306. - PubMed
-
- Yousef ZR, Redwood SR, Bucknall CA, Sulke AN, Marber MS. Late intervention after anterior myocardial infarction: effects on left ventricular size, function, quality of life, and exercise tolerance: results of The Open Artery Trial (TOAT Study) J Am Coll Cardiol. 2002;40:869–876. - PubMed
-
- Topol EJ, Califf RM, Vandormael M, Grines CL, George BS, Sanz ML, Wall T, O'Brien M, Schwaiger M, Aguirre FV. A randomized trial of late reperfusion therapy for acute myocardial infarction: Thrombolysis and Angioplasty in Myocardial Infarction-6 Study Group. Circulation. 1992;85:2090–2099. - PubMed
-
- Steg PG, Thuaire C, Himbert D, Carrie D, Champagne S, Coisne D, Khalife K, Cazaux P, Logeart D, Slama M, Spaulding C, Cohen A, Tirouvanziam A, Montely JM, Rodriguez RM, Garbarz E, Wijns W, Durand-Zaleski I, Porcher R, Brucker L, Chevret S, Chastang C. DECOPI (DEsobstruction COronaire en Post-Infarctus): a randomized multi-centre trial of occluded artery angioplasty after acute myocardial infarction. Eur Heart J. 2004;25:2187–2194. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
