

Sporadic lymphangioleiomyomatosis and tuberous sclerosis complex with lymphangioleiomyomatosis: comparison of CT features
- PMID: 17105849
- PMCID: PMC2940246
- DOI: 10.1148/radiol.2421051767
Sporadic lymphangioleiomyomatosis and tuberous sclerosis complex with lymphangioleiomyomatosis: comparison of CT features
Abstract
Purpose: To retrospectively compare the frequencies of computed tomographic (CT) findings in patients with lymphangioleiomyomatosis (LAM) and patients with tuberous sclerosis complex (TSC) and LAM.
Materials and methods: Institutional review board approval and informed consent were obtained for the HIPAA-compliant study. In 256 patients with LAM (mean age, 44 years) and 67 patients with TSC/LAM (mean age, 40 years), CT scans of the chest, abdomen, and pelvis were reviewed by a single radiologist. The fraction of lung involvement with cysts was estimated from high-spatial-resolution CT scans. Other findings assessed included noncalcified pulmonary nodules, pleural effusion, thoracic duct dilatation, hepatic and renal angiomyolipomas (AMLs), lymphangioleiomyoma (LALM), ascites, nephrectomy, and renal embolization. Confidence intervals and hypothesis tests of differences in frequencies, comparison of age quartiles, RIDIT analysis, analysis of variance, and correlation coefficients were used in the statistical analysis.
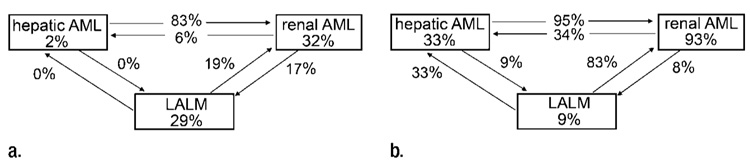
Results: Patients with LAM had more extensive lung involvement (RIDIT score, 0.36) and higher frequency of LALM (29% vs 9%, P<.001), thoracic duct dilatation (4% vs 0, P=.3), pleural effusion (12% vs 6%, P=.2), or ascites (10% vs 6%, P=.3). Patients with TSC/LAM had higher frequency of noncalcified pulmonary nodules (12% vs 1%, P<.01), hepatic (33% vs 2%, P<.001) and renal (93% vs 32%, P<.001) AMLs, nephrectomy (25% vs 7%, P<.001), or renal artery embolization (9% vs 2%, P<.05).
Conclusion: The extent of lung disease is greater in LAM than TSC/LAM. Hepatic and renal AMLs and noncalcified lung nodules are more common in TSC/LAM, while lymphatic involvement-thoracic duct dilatation, chylous pleural effusion, ascites, and LALM-is more common in LAM.
Copyright (c) RSNA, 2006.
Figures











Similar articles
-
Computed tomographic features of lymphangioleiomyomatosis: evaluation in 138 patients.Eur J Radiol. 2015 Mar;84(3):534-541. doi: 10.1016/j.ejrad.2014.12.008. Epub 2014 Dec 19. Eur J Radiol. 2015. PMID: 25544557
-
Lymphangioleiomyomatosis and multifocal micronodular pneumocyte hyperplasia in Japanese patients with tuberous sclerosis complex.Respir Investig. 2016 Jan;54(1):8-13. doi: 10.1016/j.resinv.2015.06.003. Epub 2015 Oct 29. Respir Investig. 2016. PMID: 26718139
-
CT of sclerotic bone lesions: imaging features differentiating tuberous sclerosis complex with lymphangioleiomyomatosis from sporadic lymphangioleiomymatosis.Radiology. 2010 Mar;254(3):851-7. doi: 10.1148/radiol.09090227. Radiology. 2010. PMID: 20177097 Free PMC article.
-
[Sporadic Lymphangioleiomyomatosis (sLAM) and Tuberous Sclerosis Complex (TSC) - Pulmonary Manifestations].Pneumologie. 2017 Feb;71(2):86-95. doi: 10.1055/s-0042-111522. Epub 2016 Sep 1. Pneumologie. 2017. PMID: 27585353 Review. German.
-
Lymphangioleiomyomatosis: A review.Eur J Intern Med. 2008 Jul;19(5):319-24. doi: 10.1016/j.ejim.2007.10.015. Epub 2007 Dec 26. Eur J Intern Med. 2008. PMID: 18549932 Review.
Cited by
-
Exploring the Role of Matrix Metalloproteinases as Biomarkers in Sporadic Lymphangioleiomyomatosis and Tuberous Sclerosis Complex. A Pilot Study.Front Med (Lausanne). 2021 Apr 26;8:605909. doi: 10.3389/fmed.2021.605909. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33981713 Free PMC article.
-
The effect of sirolimus on angiomyolipoma is determined by decrease of fat-poor compartments and includes striking reduction of vascular structures.Sci Rep. 2021 Apr 19;11(1):8493. doi: 10.1038/s41598-021-87930-4. Sci Rep. 2021. PMID: 33875750 Free PMC article.
-
Involvement of lymphatics in lymphangioleiomyomatosis.Lymphat Res Biol. 2009 Dec;7(4):221-8. doi: 10.1089/lrb.2009.0017. Lymphat Res Biol. 2009. PMID: 20143921 Free PMC article.
-
A 24-year-Old woman with recurrent pneumothoraces.Respir Med Case Rep. 2024 Mar 27;49:102015. doi: 10.1016/j.rmcr.2024.102015. eCollection 2024. Respir Med Case Rep. 2024. PMID: 38596619 Free PMC article.
-
Multiple cystic lung disease.Eur Respir Rev. 2015 Dec;24(138):552-64. doi: 10.1183/16000617.0046-2015. Eur Respir Rev. 2015. PMID: 26621970 Free PMC article. Review.
References
-
- Kitaichi M, Nishimura K, Itoh H, Izumi T. Pulmonary lymphangioleiomyomatosis: a report of 46 patients including a clinicopathologic study of prognostic factors. Am J Respir Crit Care Med. 1995;151:527–533. - PubMed
-
- Taylor JR, Ryu J, Colby T, Raffin T. Lymphangioleiomyomatosis: clinical course in 32 patients. N Engl J Med. 1990;323:1254–1260. - PubMed
-
- Chu SC, Horiba K, Usuki J, et al. Comprehensive evaluation of 35 patients with lymphangioleiomyomatosis. Chest. 1999;115(4):1041–1052. - PubMed
-
- Carrington CB, Cugell DW, Gaensler EA, et al. Lymphangiomyomatosis: physiologic pathologic-radiologic correlations. Am Rev Respir Dis. 1977;116:977–995. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
