

The relationship between six-month progression-free survival and 12-month overall survival end points for phase II trials in patients with glioblastoma multiforme
- PMID: 17108063
- PMCID: PMC1828103
- DOI: 10.1215/15228517-2006-025
The relationship between six-month progression-free survival and 12-month overall survival end points for phase II trials in patients with glioblastoma multiforme
Abstract
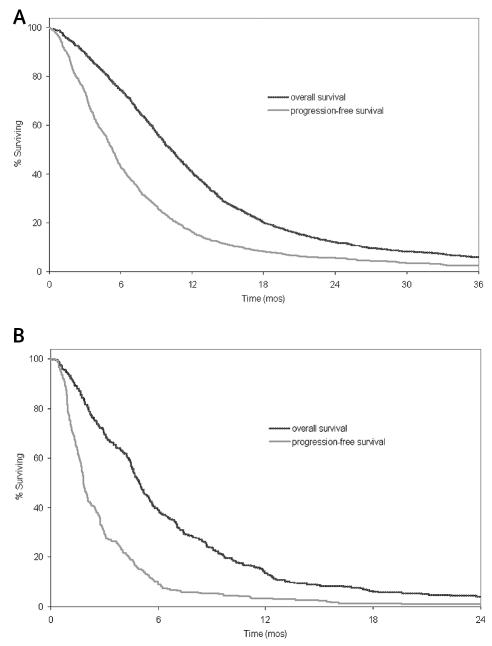
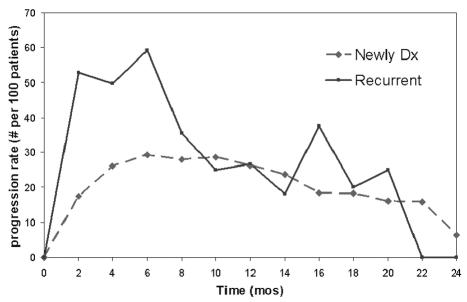
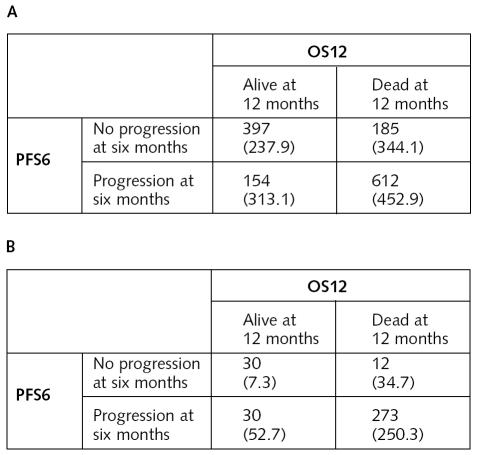
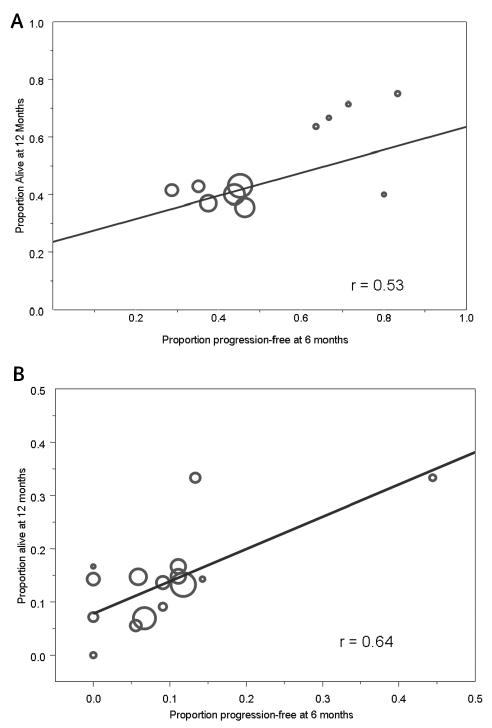
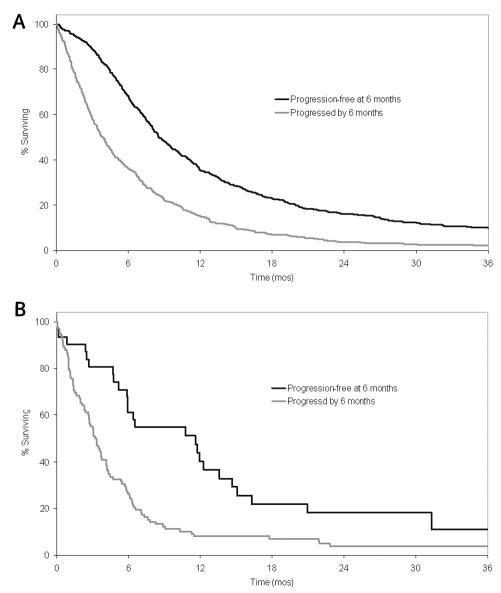
Common end points for phase II trials in patients with glioblastoma multiforme (GBM) are six-month progression-free survival (PFS6) and 12-month overall survival (OS12). OS12 can be accurately measured but may be confounded with subsequent therapies upon progression, whereas the converse is true for PFS6. Our goal was to assess the relationship between these end points separately for phase II trials in patients with newly diagnosed GBM and patients with recurrent GBM. Data were pooled from 11 North Central Cancer Treatment Group trials for patients with newly diagnosed GBM (n = 1348). All patients received radiotherapy and pharmaceutical therapy (before, during, or after radiotherapy). Data were pooled from 16 trials that used various pharmaceuticals in treating patients for recurrent GBM (n = 345). All trial regimens were declared nonefficacious by predefined criteria. Overall per-patient concordance was estimated with a kappa statistic. The relationship between OS12 and PFS6 across study arms was assessed by weighted linear regression and Pearson's correlation. Simulation was used to determine the agreement of study outcomes when using PFS6 versus OS12 end points. Cox models with progression status as a time-dependent variable and Kaplan-Meier estimators were used to ascertain the association between progression-free survival status and overall survival. At present, 97% of the patients with newly diagnosed GBM and 95% of those with recurrent GBM have died. The PFS6 and OS12 were 43% and 41%, respectively, for patients with newly diagnosed disease and 9% and 14% for patients with recurrent disease. There was only moderate concordance between the end points on both the patient level and the study level. For the simulation studies, we established phase II efficacy criteria for each end point by using the pooled estimates of OS12 (PFS6) as historical controls. The study decisions made using PFS6 and OS12 were in agreement 88% and 90% of the time for the trials of newly diagnosed and recurrent disease, respectively. Finally, there was a strong association between progression-free survival status and overall survival. PFS6 seems to be a reasonable end point for phase II trials in patients with recurrent glioblastoma.
Figures
References
-
- Batchelor T, Stanley K, Andersen J. Clinical trials in neuro-oncology. Curr Opin Neurol. 2001;14:689–694. - PubMed
-
- Begg CB, Leung DHY. On the use of surrogate end points in randomized trials. J R Stat Soc A. 2000;163(pt. 1):15–28.
-
- Brada M, Yung WKA. Clinical trial end points in malignant glioma: Need for effective trial design strategy. Semin Oncol. 2000;27(suppl. 6):11–19. - PubMed
-
- Buckner JC, Brown LD, Cascino TL, Gerstner JB, Krook JE, Westberg MW, Wiesenfeld M, O’Fallon JR, Scheithauer B. Phase II evaluation of infusional etoposide and cisplatin in patients with recurrent astrocytoma. J Neurooncol. 1990;9:249–254. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
