

Imaging and clinical characteristics of temporal bone meningioma
- PMID: 17110695
- PMCID: PMC7977196
Imaging and clinical characteristics of temporal bone meningioma
Abstract
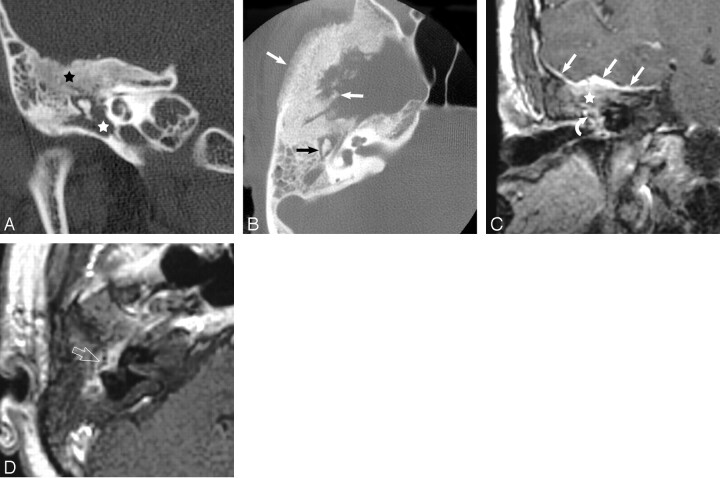
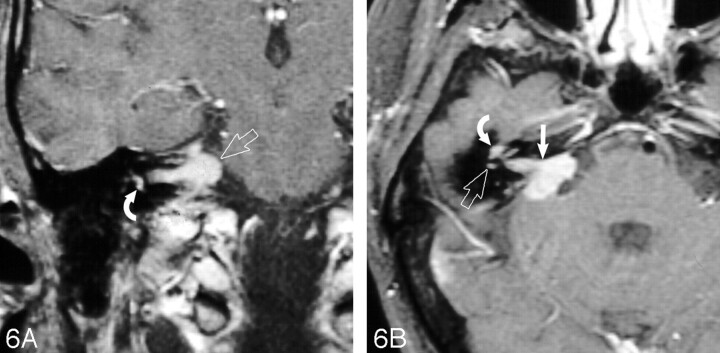
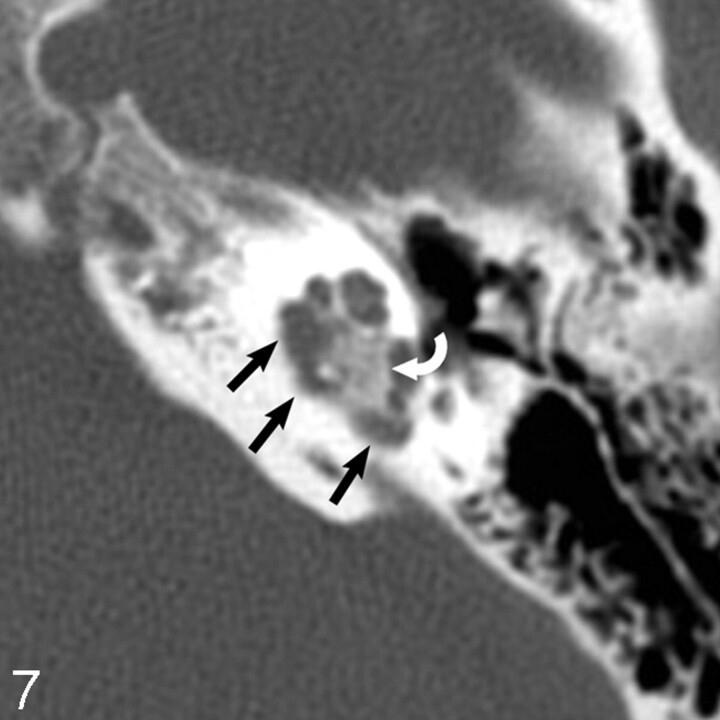
Background and purpose: Imaging characteristics of temporal bone meningioma have not been previously reported in the literature. CT and MR imaging findings in 13 cases of temporal bone meningioma are reviewed to define specific imaging features.
Methods: A retrospective review of our institutional case archive revealed 13 cases of histologically confirmed temporal bone meningioma. CT and MR imaging studies were reviewed to characterize mass location, vector of spread, bone changes, enhancement characteristics, and intracranial patterns of involvement. Clinical presenting signs and symptoms were correlated with imaging findings.
Results: Thirteen temporal bone meningiomas were reviewed in 8 women and 5 men, aged 18-65 years. Meningiomas were stratified into 3 groups on the basis of location and tumor vector of spread. There were 6 tegmen tympani, 5 jugular foramen (JF), and 2 internal auditory canal (IAC) meningiomas. Tegmen tympani and JF meningiomas were characterized by spread to the middle ear cavity. IAC meningiomas, by contrast, spread to the cochlea and vestibule. Hearing loss was the most common clinical presenting feature in all cases of temporal bone meningioma (10/13). The presence of tumor adjacent to the ossicles strongly correlated with conductive hearing loss (7/9).
Conclusion: Meningioma involving the temporal bone is rare. Three subgroups of meningioma exist in this location: tegmen tympani, JF, and IAC meningioma. Tegmen tympani and JF meningiomas spread to the middle ear cavity. IAC meningiomas spread to intralabyrinthine structures. Conductive hearing loss is commonly seen in these patients and can be surgically correctable.
Figures




References
-
- Prayson RA. Middle ear meningiomas. Ann Diag Pathol 2000;4:149–53 - PubMed
-
- Macdonald AJ, Salzman KL, Harnsberger HR, et al. Primary jugular foramen meningioma: imaging appearance and differentiating features. AJR Am J Roentgenol 2004;182:373–77 - PubMed
-
- Thompson LD, Bouffard JP, Sandberg GD, et al. Primary ear and temporal bone meningiomas: a clinicopathologic study of 36 cases with a review of the literature. Mod Pathol 2003;16:236–45 - PubMed
-
- Rosahl SK, Mirzayan MJ, Samii M. Osteolytic intra-osseous meningiomas: illustrated review. Acta Neurochir (Wien) 2004;146:1245–49. Epub 2004 Sep 9 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical