

Is shared care with annual hospital review better value for money than predominantly hospital-based care in patients with established stable rheumatoid arthritis?
- PMID: 17124249
- PMCID: PMC1954606
- DOI: 10.1136/ard.2006.061234
Is shared care with annual hospital review better value for money than predominantly hospital-based care in patients with established stable rheumatoid arthritis?
Abstract
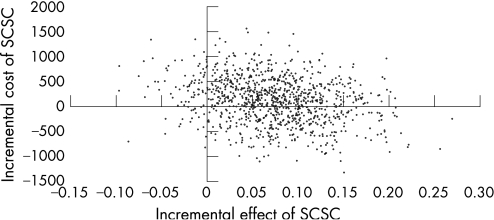
Objective: To assess the cost effectiveness and cost effectiveness acceptability of symptom control delivered by shared care (SCSC) and aggressive treatment delivered in hospital (ATH) for established rheumatoid arthritis (RA).
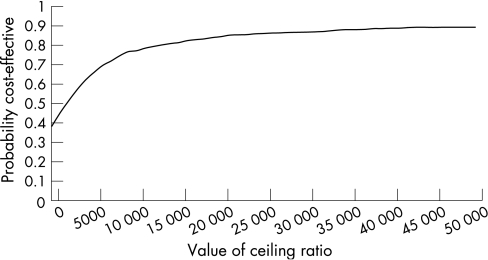
Methods: Economic data were collected within the British Rheumatoid Outcome Study Group randomised controlled trial of SCSC and ATH. A broad perspective was used (UK National Health Service, social support services and patients). Cost per quality adjusted life year (QALY) gained, net benefit statistics and cost effectiveness acceptability curves were estimated. Costs and outcomes were discounted at 3.5%. Sensitivity analysis tested the robustness of the results to analytical assumptions.
Results: The mean (SD) cost per person was 4540 pounds (4700) in the SCSC group and 4440 pounds (4900) in the ATH group. The mean (SD) QALYs per person for 3 years were 1.67 (0.56) in the SCSC group and 1.60 (0.60) in the ATH group. If decision makers are prepared to pay > or = 2000 pounds to gain 1 QALY, SCSC is likely to be cost effective in 60-90% of cases.
Conclusions: The primary economic analysis and sensitivity analyses indicate that SCSC is likely to be more cost effective than ATH in 60-90% of cases. This result seems to be robust to assumptions required by the analysis. This study is one of a limited number of randomised controlled trials to collect detailed resource use and health status data and estimate the costs and QALYs of treatment for established RA. This trial is one of the largest RA studies to use the EuroQol.
Conflict of interest statement
Competing interests: None declared.
References
-
- van Gestel A M, Stucki G. Evaluation of established rheumatoid arthritis. Baillieres Best Pract Res Clin Rheumatol 199913629–644. - PubMed
-
- Anderson J J, Wells G, Verhoeven A C, Felson D T. Factors predicting response to treatment in rheumatoid arthritis: the importance of disease duration. Arthritis Rheum 20004322–29. - PubMed
-
- Fries J F, Williams C A, Morfeld D, Singh G, Sibley J. Reduction in long‐term disability in patients with rheumatoid arthritis by disease‐modifying antirheumatic drug‐based treatment strategies. Arthritis Rheum 199639616–622. - PubMed
-
- Wolfe F, Hawley D J, Cathey M A. Termination of slow acting antirheumatic therapy in rheumatoid arthritis: a 14‐year prospective evaluation of 1017 consecutive starts. J Rheumatol 199017994–1002. - PubMed
-
- Morand E F, McCloud P I, Littlejohn G O. Life table analysis of 879 treatment episodes with slow acting antirheumatic drugs in community rheumatology practice. J Rheumatol 199219704–708. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
