

Population pharmacokinetics of artesunate and dihydroartemisinin following intra-rectal dosing of artesunate in malaria patients
- PMID: 17132053
- PMCID: PMC1664603
- DOI: 10.1371/journal.pmed.0030444
Population pharmacokinetics of artesunate and dihydroartemisinin following intra-rectal dosing of artesunate in malaria patients
Abstract
Background: Intra-rectal artesunate has been developed as a potentially life-saving treatment of severe malaria in rural village settings where administration of parenteral antimalarial drugs is not possible. We studied the population pharmacokinetics of intra-rectal artesunate and the relationship with parasitological responses in patients with moderately severe falciparum malaria.
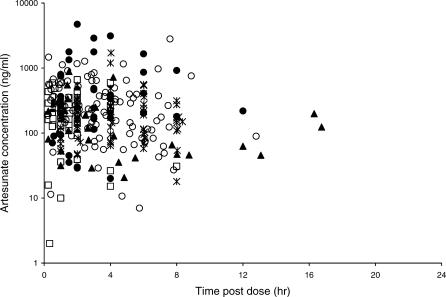
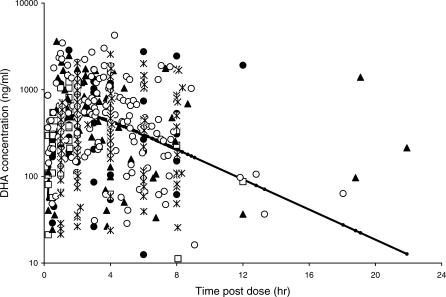
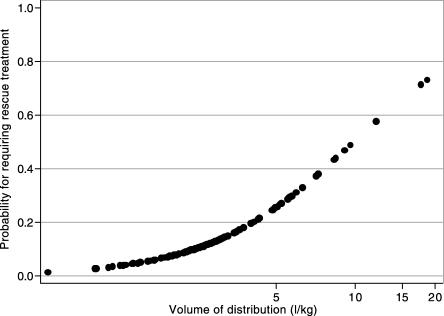
Methods and findings: Adults and children in Africa and Southeast Asia with moderately severe malaria were recruited in two Phase II studies (12 adults from Southeast Asia and 11 children from Africa) with intensive sampling protocols, and three Phase III studies (44 children from Southeast Asia, and 86 children and 26 adults from Africa) with sparse sampling. All patients received 10 mg/kg artesunate as a single intra-rectal dose of suppositories. Venous blood samples were taken during a period of 24 h following dosing. Plasma artesunate and dihydroartemisinin (DHA, the main biologically active metabolite) concentrations were measured by high-performance liquid chromatography with electrochemical detection. The pharmacokinetic properties of DHA were determined using nonlinear mixed-effects modelling. Artesunate is rapidly hydrolysed in vivo to DHA, and this contributes the majority of antimalarial activity. For DHA, a one-compartment model assuming complete conversion from artesunate and first-order appearance and elimination kinetics gave the best fit to the data. The mean population estimate of apparent clearance (CL/F) was 2.64 (l/kg/h) with 66% inter-individual variability. The apparent volume of distribution (V/F) was 2.75 (l/kg) with 96% inter-individual variability. The estimated DHA population mean elimination half-life was 43 min. Gender was associated with increased mean CL/F by 1.14 (95% CI: 0.36-1.92) (l/kg/h) for a male compared with a female, and weight was positively associated with V/F. Larger V/Fs were observed for the patients requiring early rescue treatment compared with the remainder, independent of any confounders. No associations between the parasitological responses and the posterior individual estimates of V/F, CL/F, and AUC0-6h were observed.
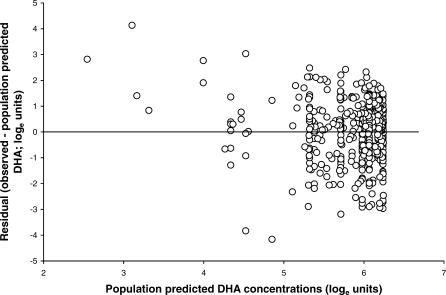
Conclusions: The pharmacokinetic properties of DHA were affected only by gender and body weight. Patients with the lowest area under the DHA concentration curve did not have slower parasite clearance, suggesting that rectal artesunate is well absorbed in most patients with moderately severe malaria. However, a number of modelling assumptions were required due to the large intra- and inter-individual variability of the DHA concentrations.
Conflict of interest statement
Figures

Similar articles
-
Disposition of artesunate and dihydroartemisinin after administration of artesunate suppositories in children from Papua New Guinea with uncomplicated malaria.Antimicrob Agents Chemother. 2004 Aug;48(8):2966-72. doi: 10.1128/AAC.48.8.2966-2972.2004. Antimicrob Agents Chemother. 2004. PMID: 15273107 Free PMC article. Clinical Trial.
-
Artesunate suppositories versus intramuscular artemether for treatment of severe malaria in children in Papua New Guinea.Antimicrob Agents Chemother. 2006 Mar;50(3):968-74. doi: 10.1128/AAC.50.3.968-974.2006. Antimicrob Agents Chemother. 2006. PMID: 16495259 Free PMC article. Clinical Trial.
-
Pharmacokinetics/Pharmacodynamics findings after repeated administration of ARTESUNATE thermostable suppositories (RECTOCAPS) in Vietnamese patients with uncomplicated malaria.Eur J Drug Metab Pharmacokinet. 2006 Jan-Mar;31(1):41-5. doi: 10.1007/BF03190641. Eur J Drug Metab Pharmacokinet. 2006. PMID: 16715782 Clinical Trial.
-
Rectal artemisinins for malaria: a review of efficacy and safety from individual patient data in clinical studies.BMC Infect Dis. 2008 Mar 28;8:39. doi: 10.1186/1471-2334-8-39. BMC Infect Dis. 2008. PMID: 18373841 Free PMC article. Review.
-
Systematic review of artesunate pharmacokinetics: Implication for treatment of resistant malaria.Int J Infect Dis. 2019 Dec;89:30-44. doi: 10.1016/j.ijid.2019.08.030. Epub 2019 Sep 3. Int J Infect Dis. 2019. PMID: 31491558
Cited by
-
Prereferral rectal artesunate and referral completion among children with suspected severe malaria in the Democratic Republic of the Congo, Nigeria and Uganda.BMJ Glob Health. 2022 May;7(5):e008346. doi: 10.1136/bmjgh-2021-008346. BMJ Glob Health. 2022. PMID: 35580913 Free PMC article.
-
Rectal artesunate suppositories for the pre-referral treatment of suspected severe malaria.PLoS Med. 2023 Nov 9;20(11):e1004312. doi: 10.1371/journal.pmed.1004312. eCollection 2023 Nov. PLoS Med. 2023. PMID: 37943884 Free PMC article.
-
Parasite Clearance and Artemether Pharmacokinetics Parameters Over the Course of Artemether-Lumefantrine Treatment for Malaria in Human Immunodeficiency Virus (HIV)-Infected and HIV-Uninfected Ugandan Children.Open Forum Infect Dis. 2016 Dec 15;3(4):ofw217. doi: 10.1093/ofid/ofw217. eCollection 2016 Oct. Open Forum Infect Dis. 2016. PMID: 28018925 Free PMC article.
-
Continued cytoadherence of Plasmodium falciparum infected red blood cells after antimalarial treatment.Mol Biochem Parasitol. 2010 Feb;169(2):71-8. doi: 10.1016/j.molbiopara.2009.09.007. Epub 2009 Oct 1. Mol Biochem Parasitol. 2010. PMID: 19800372 Free PMC article.
-
The sensitivity of artesunate against Schistosoma japonicum decreased after 10 years of use in China.Parasitol Res. 2010 Sep;107(4):873-8. doi: 10.1007/s00436-010-1944-5. Epub 2010 Jun 15. Parasitol Res. 2010. PMID: 20549236 Clinical Trial.
References
-
- Dorndrop A, Nosten F, Stepniewska N, Day NP, White NJ. Artesunate versus quinine for treatment of severe falciparum malaria: A randomised trial. Lancet. 2005;366:717–725. - PubMed
-
- Li GQ. Guo XB, editor. Clinical studies on artemisinin suppositories, artesunate and artemether. Clinical trials on Qinghaosu and its derivatives. Volume 1. 1990.
-
- Arnold K, Tran TH, Nguyen TC, Nguyen HP, Pham P. A randomised comparative study of artemisininine (qinghaosu) suppositories and oral quinine in acute falciparum malaria. Trans R Soc Trop Med Hyg. 1990;84:499–502. - PubMed
-
- Cao XT, Bethell DB, Pham TP, Ta TT, Tran TN, et al. Comparison of artemisinin suppositories, intramuscular artesunate and intravenous quinine for the treatment of severe childhood malaria. Trans R Soc Trop Med Hyg. 1997;91:335–342. - PubMed
-
- Hien TT, Tam DT, Cuc NT, Arnold K. Comparative effectiveness of artemisinin suppositories and oral quinine in children with acute falciparum malaria. Trans R Soc Trop Med Hyg. 1991;85:210–211. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
