

Withdrawal from long-term benzodiazepine use: randomised trial in family practice
- PMID: 17132385
- PMCID: PMC1934057
Withdrawal from long-term benzodiazepine use: randomised trial in family practice
Abstract
Background: The long-term use of benzodiazepines is highly prevalent in developed societies and is not devoid of risks. Withdrawing patients from these drugs is often difficult. Tapering off benzodiazepines has been shown to be a good strategy for discontinuing their long-term use.
Aim: To establish the efficacy of an intervention programme for reducing the chronic use of benzodiazepines.
Design of study: Randomised, two-arm, parallel, non-blinded controlled trial.
Setting: Three urban healthcare centres covering a population of 50,000 inhabitants (Mallorca, Spain).
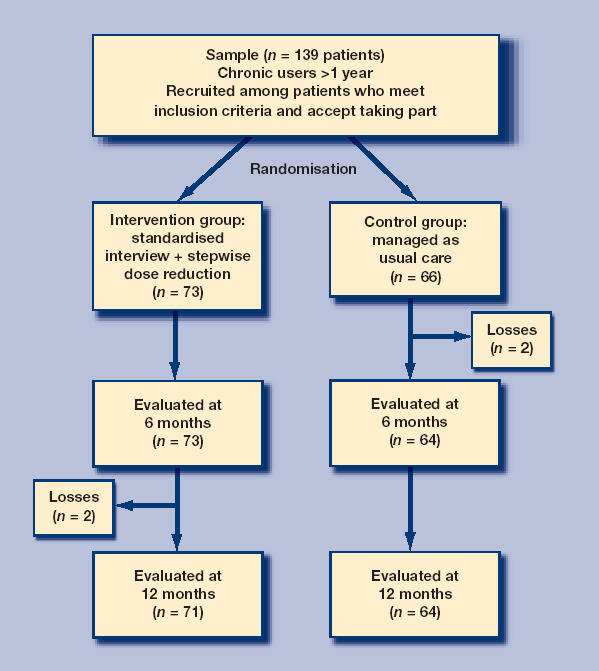
Method: Adult patients (n = 139) taking benzodiazepines daily for more than a year and visited by their family physician were randomised into an intervention group (n = 73) that received standardised advice and a tapering off schedule with biweekly follow-up visits, or into a control group (n = 66), that was managed following routine clinical practice. Both were followed for a year.
Results: Patients achieved withdrawal or reduced their dose by at least 50% after 6 and 12 months. Abstinence and withdrawal symptoms were also measured. Both groups were homogeneous for personal, clinical and psychological characteristics and for benzodiazepine use. Only two patients from each group were lost to follow-up. After 12 months, 33 (45.2%) patients in the intervention group and six (9.1%) in the control group had discontinued benzodiazepine use; relative risk = 4.97 (95% confidence interval [CI] = 2.2 to 11.1), absolute risk reduction = 0.36 (95% CI = 0.22 to 0.50). For every three interventions, one patient achieved withdrawal. Sixteen (21.9%) subjects from the intervention group and 11 (16.7%) controls reduced their initial dose by more than 50%.
Conclusion: Standardised advice given by the family physician, together with a tapering off schedule, is effective for withdrawing patients from long-term benzodiazepine use and is feasible in primary care.
Comment in
-
Z-drugs.Br J Gen Pract. 2007 Mar;57(536):246. Br J Gen Pract. 2007. PMID: 17359622 Free PMC article. No abstract available.
References
-
- Rayon P, Montero D, Santamaría B. Benzodiazepine consumption in Spain. Eur J Clin Pharmacol. 1997;52(4):321–323. - PubMed
-
- Herings RM, Stricker BH, De Boer A. Benzodiazepines and the risk of falling leading to femur fractures. Dosage more important than elimination half-life. Arch Intern Med. 1995;155(16):1801–1807. - PubMed
-
- National Health Committee. Guidelines for assessing and treating anxiety disorders. Wellington (New Zealand): National Health Committee; 1998.
-
- Estivill E, Bové A, García-Borreguero D. Consensus on drug treatment, definition and diagnosis for insomnia. Clin Drug Invest. 2003;23:351–385. - PubMed
-
- Cañellas F, Ochogavía J, Llobera J, et al. Trastornos del sueño y consumo de hipnóticos en la Isla de Mallorca [Sleep disorders and the consumption of hypnotics on the island of Mallorca] Rev Clín Esp. 1998;198:719–725. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials