

Results of the randomized international FAB/LMB96 trial for intermediate risk B-cell non-Hodgkin lymphoma in children and adolescents: it is possible to reduce treatment for the early responding patients
- PMID: 17132719
- PMCID: PMC1852229
- DOI: 10.1182/blood-2006-07-036673
Results of the randomized international FAB/LMB96 trial for intermediate risk B-cell non-Hodgkin lymphoma in children and adolescents: it is possible to reduce treatment for the early responding patients
Abstract
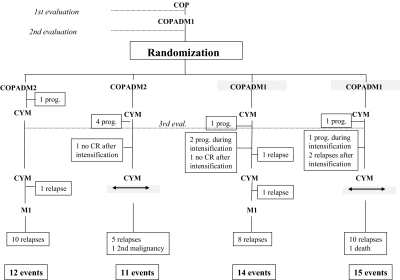
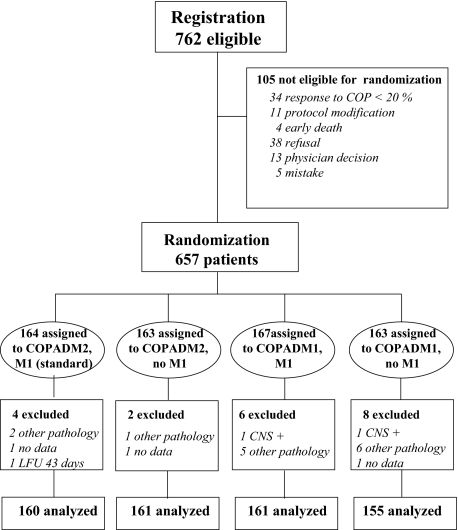
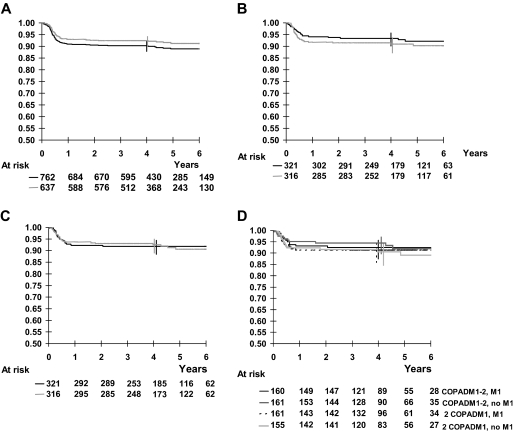
A previous study (LMB89) of the French Society of Pediatric Oncology for childhood mature B-cell lymphoma (B-NHL) demonstrated a 92% 3-year event-free survival (EFS) for intermediate-risk group B defined as "non-resected" stage II/I and CNS-negative advanced-stage IIV/IV (70% of cases). We performed the FAB/LMB96 trial to assess the possibility of reducing treatment in children/adolescents with intermediate-risk B-NHL without jeopardizing survival. "Early responding" patients (tumor response > 20% at day 7) were randomized in a factorial design between 4 arms, 2 receiving half-dose of cyclophosphamide in the second induction course with cyclophosphamide, Oncovin (vincristine), prednisone, Adriamycin (doxorubicin), methotrexate (COPADM) and 2 not receiving the maintenance course M1. A total of 657 patients were randomized (May 1996 to June 2001) and 637 were analyzed. The analysis showed no significant effect of any of the treatment reductions on EFS and survival. The 4-year EFS was 93.4% and 90.9% in the groups with full-dose and half-dose of cyclophosphamide (RR = 1.3, P = .40) and 91.9% and 92.5% in the groups with and without M1 (RR = 1.01, P = .98). There was no interaction between the 2 treatment reductions or between each treatment reduction and LDH level or histologic subtypes (Burkitt/Burkitt-like or large B-cell). Children/adolescents with intermediate-risk B-NHL who have an early response and achieve a complete remission after the first consolidation course can be cured with a 4-course treatment with a total dose of only 3.3 g/m2 cyclophosphamide and 120 mg/m2 doxorubicin.
Figures
References
-
- Patte C, Philip T, Rodary C, et al. Improved survival rate in children with stage III and IV B cell non-Hodgkin's lymphoma and leukemia using multi-agent chemotherapy: results of a study of 114 children from the French Pediatric Oncology Society. J Clin Oncol. 1986;4:1219–1226. - PubMed
-
- Bowman WP, Shuster JJ, Cook B, et al. Improved survival for children with B-cell acute lymphoblastic leukemia and stage IV small noncleaved-cell lymphoma: a pediatric oncology group study. J Clin Oncol. 1996;14:1252–1261. - PubMed
-
- Patte C, Philip T, Rodary C, et al. High survival rate in advanced-stage B-cell lymphomas and leukemias without CNS involvement with a short intensive polychemotherapy: results from the French Pediatric Oncology Society of a randomized trial of 216 children. J Clin Oncol. 1991;9:123–132. - PubMed
-
- Magrath I, Adde M, Shad A, et al. Adults and children with small non-cleaved-cell lymphoma have a similar excellent outcome when treated with the same chemotherapy regimen. J Clin Oncol. 1996;14:925–934. - PubMed
-
- Sullivan MP, Brecher M, Ramirez I, et al. High-dose cyclophosphamide-high-dose methotrexate with coordinated intrathecal therapy for advanced nonlymphoblastic lymphoma of childhood: results of a Pediatric Oncology Group study. Am J Pediatr Hematol Oncol. 1991;13:288–295. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
