

Safety, tolerability and efficacy of levodopa-carbidopa treatment for cocaine dependence: two double-blind, randomized, clinical trials
- PMID: 17134849
- PMCID: PMC2693095
- DOI: 10.1016/j.drugalcdep.2006.10.011
Safety, tolerability and efficacy of levodopa-carbidopa treatment for cocaine dependence: two double-blind, randomized, clinical trials
Abstract
Rationale: The role of dopamine in cocaine abuse has been long recognized. Cocaine use can profoundly alter dopaminergic functioning through depletion of this monoamine and changes in receptor functioning. Based on these facts, levodopa (L-dopa) pharmacotherapy may be helpful in reducing or abolishing cocaine use.
Objective: The current studies sought to evaluate the safety, tolerability and efficacy of L-dopa as a treatment for cocaine dependence.
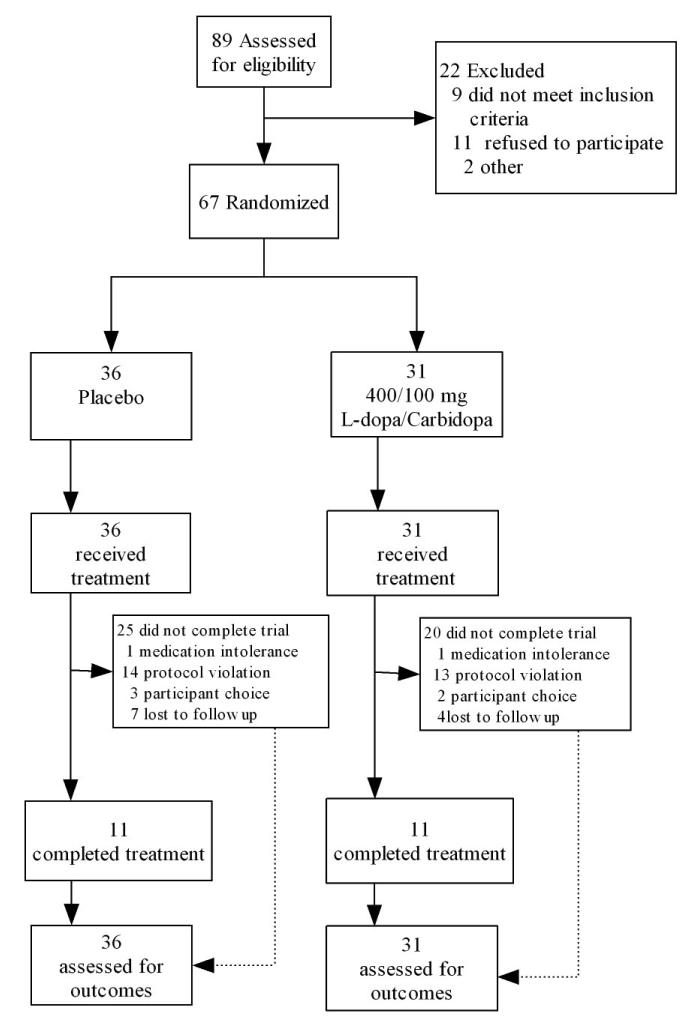
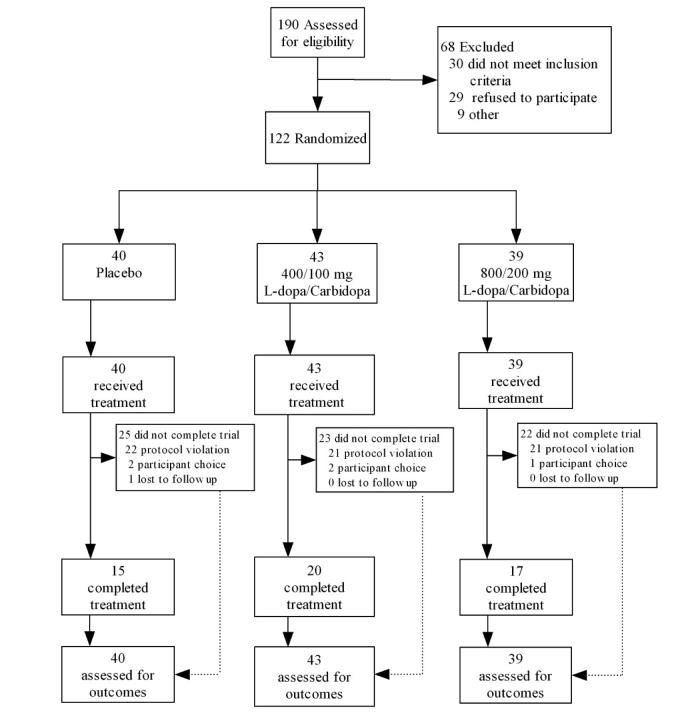
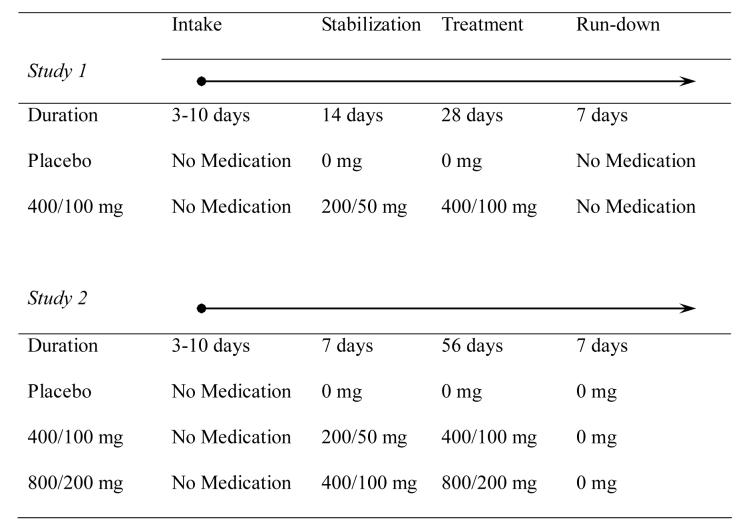
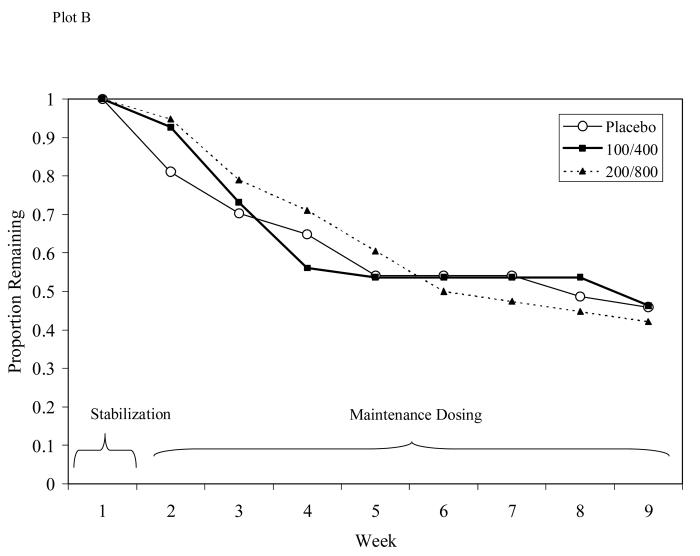
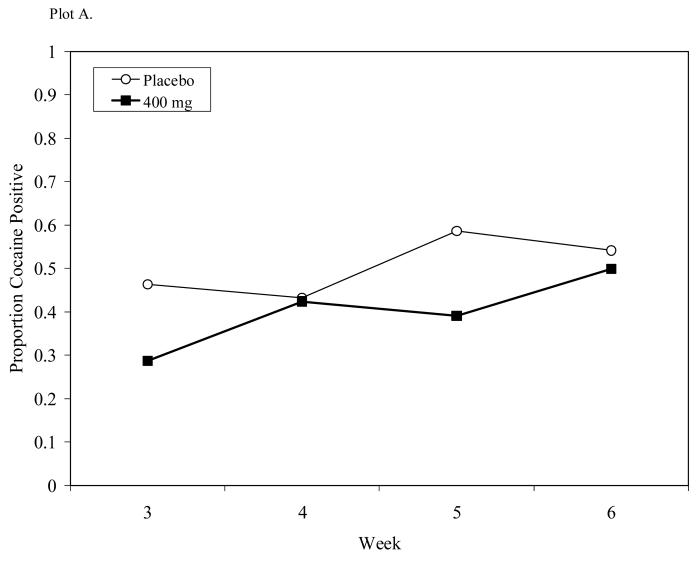
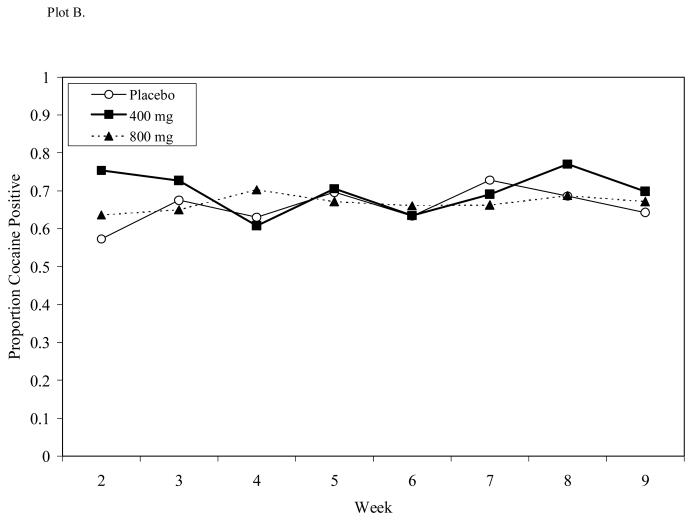
Methods: In Study 1, 67 cocaine-dependent subjects were randomized in a 5-week, double-blind, placebo-controlled safety trial. Subjects received either placebo, or 400 mg L-dopa plus 100 mg of the peripheral decarboxylase inhibitor, carbidopa, in a sustained-release preparation (Sinemet CR). In Study 2, 122 cocaine-dependent subjects were enrolled in a 9-week, randomized, double-blind, placebo-controlled trial to compare placebo to 400/100 mg and 800/200 mg L-dopa/carbidopa treatments. Placebo or L-dopa were administered twice daily in both studies.
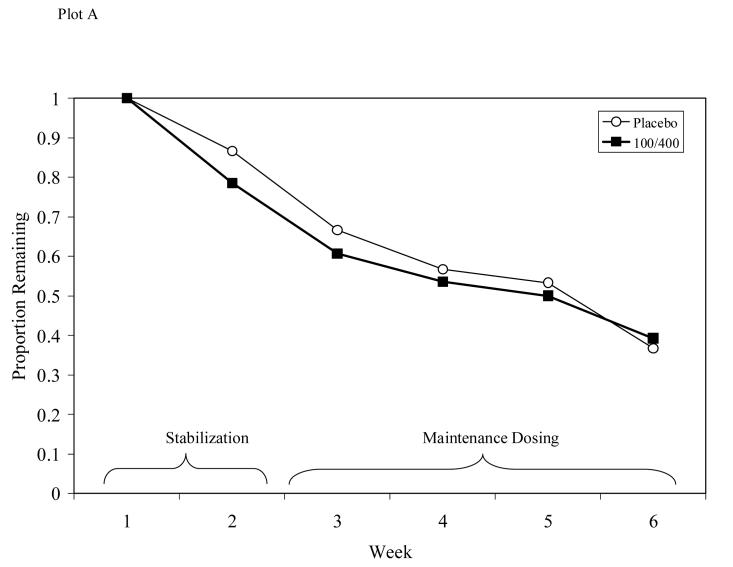
Results: L-dopa was well tolerated with similar retention and medication adherence rates compared to placebo. Only two side effects occurred more often in L-dopa-treated patients: nausea and dizziness. L-dopa lowered diastolic blood pressure in a dose-dependent fashion. In these trials, L-dopa had no effect on cocaine use, cocaine craving, or mood.
Conclusion: These two studies demonstrate the safety and tolerability of L-dopa pharmacotherapy in cocaine-dependent patients. No evidence for greater efficacy of L-dopa compared to placebo was observed. The possibility of enhancing treatment effects by combining L-dopa with other behavioral or pharmacological interventions is discussed.
Figures
References
-
- Batki SL, Washburn AM, Delucchi K, Jones RT. A controlled trial of fluoxetine in crack cocaine dependence. Drug Alcohol Depend. 1996;41:137–142. - PubMed
-
- Bavry JL. STAT-POWER. Scientific Software International, Incorporated; Chicago, IL: 1993.
-
- Beck A, Ward C, Mendelson M, Mack J, Erbaugh J. An inventory of measuring depression. Archives of General Psychiatry. 1961;49:599–608. - PubMed
-
- Bergman J, Kamien JB, Spealman RD. Antagonism of cocaine self-administration by selective dopamine D(1) and D(2) antagonists. Behav Pharmacol. 1990;1:355–363. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
