

Expression of antibodies directed to Paracoccidioides brasiliensis glycosphingolipids during the course of paracoccidioidomycosis treatment
- PMID: 17135452
- PMCID: PMC1797792
- DOI: 10.1128/CVI.00285-06
Expression of antibodies directed to Paracoccidioides brasiliensis glycosphingolipids during the course of paracoccidioidomycosis treatment
Abstract
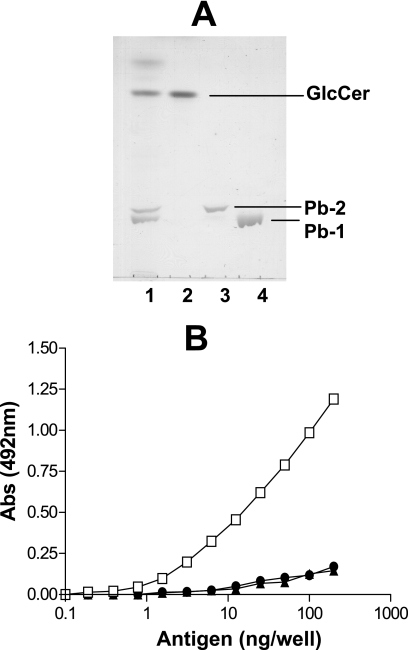
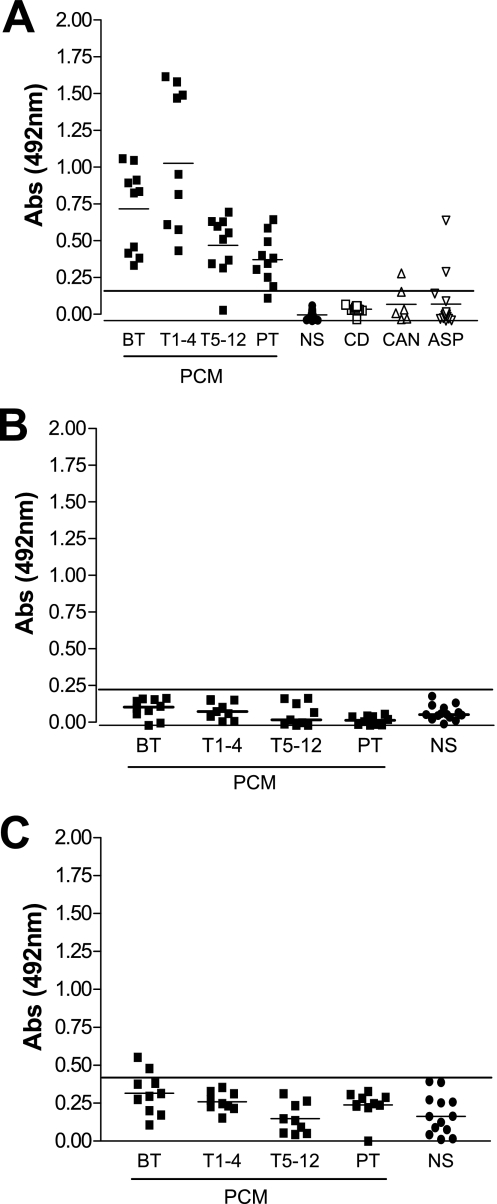
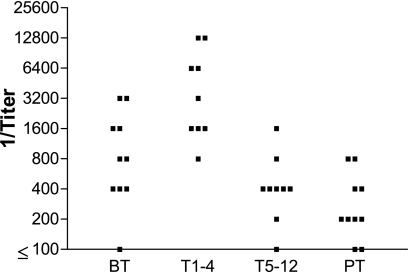
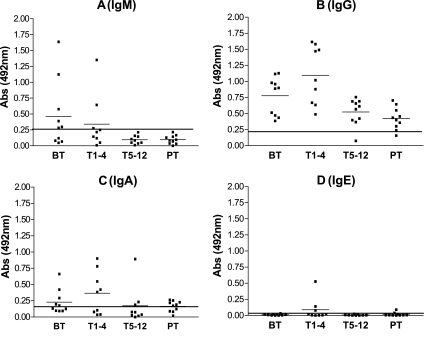
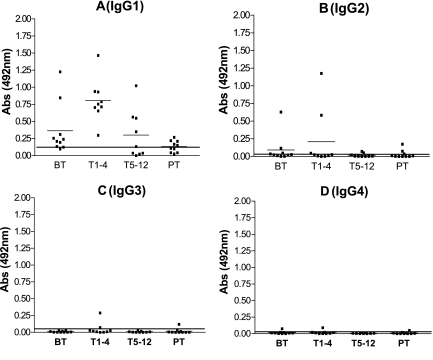
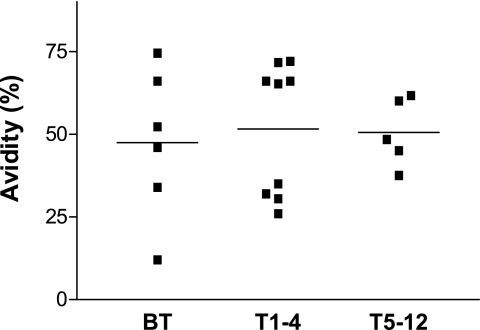
Paracoccidioidomycosis (PCM) is a granulomatous disease caused by the dimorphic fungus Paracoccidioides brasiliensis. The immunoglobulin classes and isotypes of antibodies directed to acidic glycosphingolipids (GSLs) and glucosylceramide of P. brasiliensis were determined by enzyme-linked immunosorbent assay of sera from 31 PCM patients. The reactivities of 38 serum samples were analyzed by considering the stage of treatment: before antifungal treatment (n = 10), during 1 to 4 months of treatment (T1-4; n = 9), during 5 to 12 months of treatment (T5-12; n = 9), and posttreatment (PT; n = 10). Sera from healthy subjects (n = 12) were used as controls. Only the GSL Pb-1 antigen, which presents the carbohydrate structure Galfbeta1-6(Manalpha1-3)Manbeta1, was reactive with the PCM patient sera. The PCM patient sera did not react with Pb-2, which lacks the Galf residue and which is considered the biosynthetic precursor of Pb-1, indicating that the Galf residue is essential for antibody reactivity. The Pb-1 glycolipid from nontreated patients elicited a primary immune response with immunoglobulin M (IgM) production and subsequent switching to IgG1 production. The IgG1 titer increased after the start of antifungal treatment (T1-4 group), and general decreases in the anti-Pb-1 antibody titers were observed after 5 months of treatment (T5-12 and PT groups). The Pb-1 antigen, an acidic GSL with terminal Galf residue, has potential application as an elicitor of the host immune response in patients with PCM.
Figures
References
-
- Baida, H., P. J. C. Biselli, M. Juvenale, G. J. S. Del Negro, M. J. S. Mendes-Giannini, A. J. S. Duarte, and G. Benard. 1999. Differential antibody isotype expression to the major Paracoccidioides brasiliensis antigen in juvenile and adult form paracoccidioidomycosis. Microbes Infect. 1:273-278. - PubMed
-
- Biselli, P. J. C., M. Juvenale, M. J. S. Mendes-Giannini, A. J. S. Durte, and G. Benard. 2001. IgE antibody response to the main component of Paracoccidioides brasiliensis in patient with paracoccidioidomycosis. Med. Mycol. 39:475-478. - PubMed
-
- De Camargo, Z. P., and M. F. Franco. 2000. Current knowledge on pathogenesis and immunodiagnosis of paracoccidioidomycosis. Rev. Iberoam. Micol. 17:41-48. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
