

Male circumcision, religion, and infectious diseases: an ecologic analysis of 118 developing countries
- PMID: 17137513
- PMCID: PMC1764746
- DOI: 10.1186/1471-2334-6-172
Male circumcision, religion, and infectious diseases: an ecologic analysis of 118 developing countries
Abstract
Background: Both religious practices and male circumcision (MC) have been associated with HIV and other sexually-transmitted infectious diseases. Most studies have been limited in size and have not adequately controlled for religion, so these relationships remain unclear.
Methods: We evaluated relationships between MC prevalence, Muslim and Christian religion, and 7 infectious diseases using country-specific data among 118 developing countries. We used multivariate linear regression to describe associations between MC and cervical cancer incidence, and between MC and HIV prevalence among countries with primarily sexual HIV transmission.
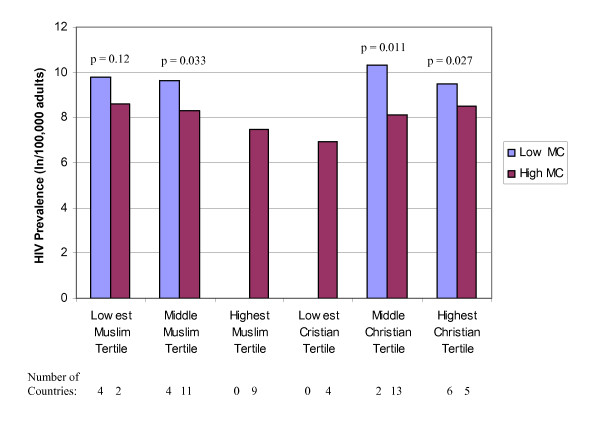
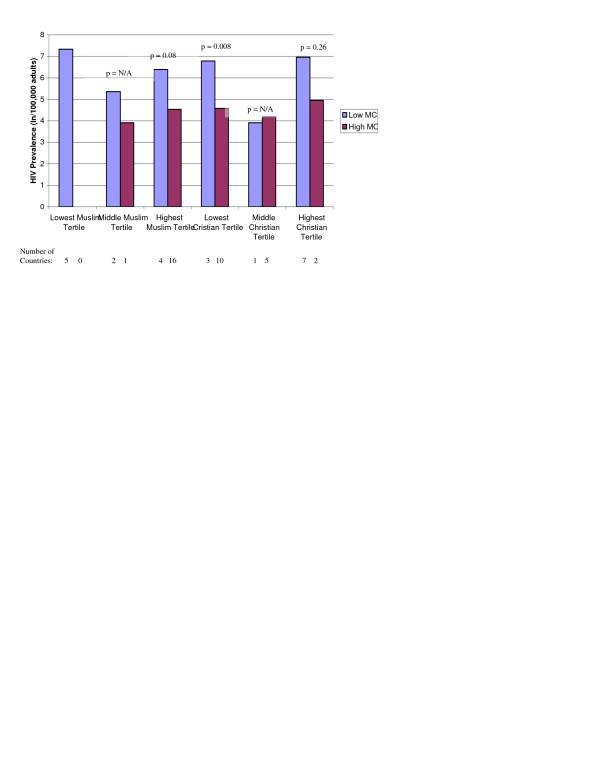
Results: Fifty-three, 14, and 51 developing countries had a high (>80%), intermediate (20-80%), and low (<20%) MC prevalence, respectively. In univariate analyses, MC was associated with lower HIV prevalence and lower cervical cancer incidence, but not with HSV-2, syphilis, nor, as expected, with Hepatitis C, tuberculosis, or malaria. In multivariate analysis after stratifying the countries by religious groups, each categorical increase of MC prevalence was associated with a 3.65/100,000 women (95% CI 0.54-6.76, p = 0.02) decrease in annual cervical cancer incidence, and a 1.84-fold (95% CI 1.36-2.48, p < 0.001) decrease in the adult HIV prevalence among sub-Saharan African countries. In separate multivariate analyses among non-sub-Saharan African countries controlling for religion, higher MC prevalence was associated with a 8.94-fold (95% CI 4.30-18.60) decrease in the adult HIV prevalence among countries with primarily heterosexual HIV transmission, but not, as expected, among countries with primarily homosexual or injection drug use HIV transmission (p = 0.35).
Conclusion: Male circumcision was significantly associated with lower cervical cancer incidence and lower HIV prevalence in sub-Saharan Africa, independent of Muslim and Christian religion. As predicted, male circumcision was also strongly associated with lower HIV prevalence among countries with primarily heterosexual HIV transmission, but not among countries with primarily homosexual or injection drug use HIV transmission. These findings strengthen the reported biological link between MC and some sexually transmitted infectious diseases, including HIV and cervical cancer.
Figures

References
-
- Caldwell JC, Caldwell P. The African AIDS epidemic. Sci Am. 1996;274:62–3. - PubMed
-
- Carael M, Buvé A, Awusabo-Asare K. The making of HIV epidemics: What are the driving forces? AIDS. 1997;2:185–205. - PubMed
-
- Auvert B, Buvé A, Ferry B, Carael M, Morison L, Lagarde E, Robinson NJ, Kahindo M, Chege J, Rutenberg N, Musonda R, Laourou M, Akam E, Study Group on the Heterogeneity of HIV Epidemics in African Cities Ecological and individual level analysis of risk factors for HIV infection in four urban populations in sub-Saharan Africa with different levels of HIV infection. AIDS. 2001;15:S15–S30. doi: 10.1097/00002030-200108004-00003. - DOI - PubMed
-
- Auvert B, Ferry B. Modeling the spread of HIV infection in four cities of sub-Saharan Africa [abstract] Presented at XIV International AIDS Conference, 2002; Barcelona;
-
- Drain PK, Smith JS, Hughes JP, Halperin DT, Holmes KK. Correlates of national HIV seroprevalence. An ecological analysis of 122 developing countries. J Acquir Immune Defic Syndr. 2004;35:407–420. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
