

Lung dosimetry for radioiodine treatment planning in the case of diffuse lung metastases
- PMID: 17138741
- PMCID: PMC2967027
Lung dosimetry for radioiodine treatment planning in the case of diffuse lung metastases
Abstract
The lungs are the most frequent sites of distant metastasis in differentiated thyroid carcinoma. Radioiodine treatment planning for these patients is usually performed following the Benua-Leeper method, which constrains the administered activity to 2.96 GBq (80 mCi) whole-body retention at 48 h after administration to prevent lung toxicity in the presence of iodine-avid lung metastases. This limit was derived from clinical experience, and a dosimetric analysis of lung and tumor absorbed dose would be useful to understand the implications of this limit on toxicity and tumor control. Because of highly nonuniform lung density and composition as well as the nonuniform activity distribution when the lungs contain tumor nodules, Monte Carlo dosimetry is required to estimate tumor and normal lung absorbed dose. Reassessment of this toxicity limit is also appropriate in light of the contemporary use of recombinant thyrotropin (thyroid-stimulating hormone) (rTSH) to prepare patients for radioiodine therapy. In this work we demonstrated the use of MCNP, a Monte Carlo electron and photon transport code, in a 3-dimensional (3D) imaging-based absorbed dose calculation for tumor and normal lungs.
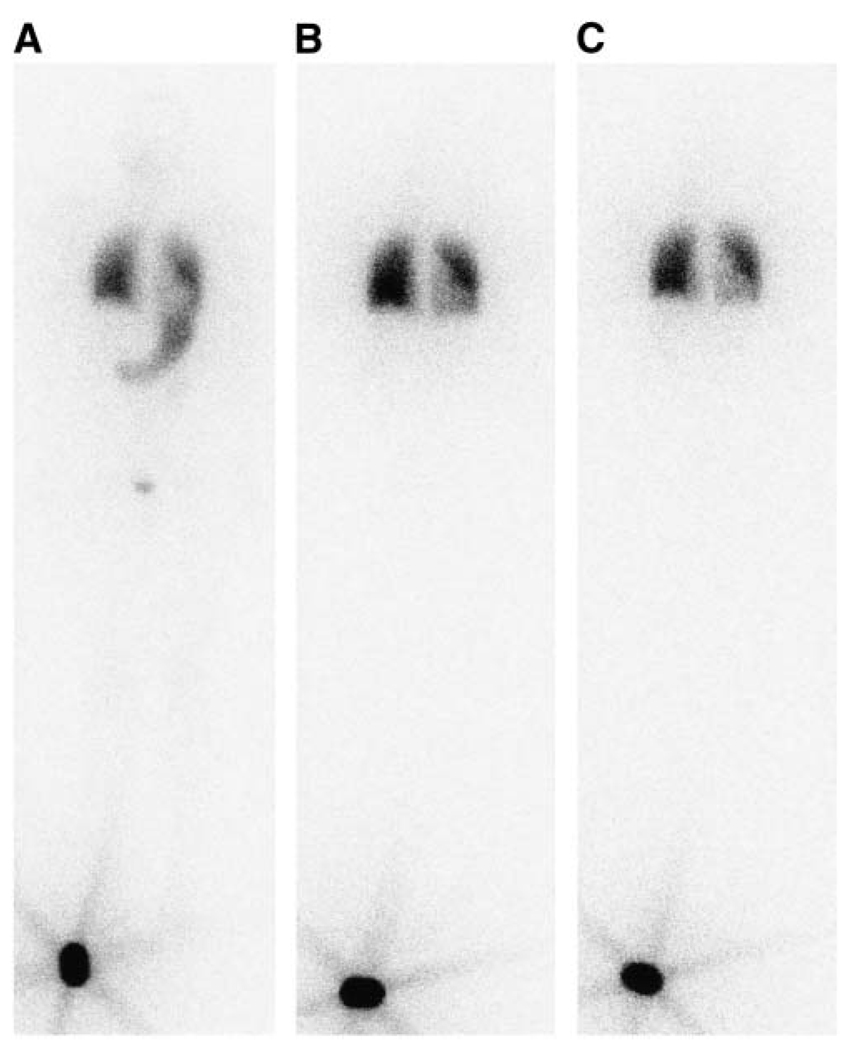
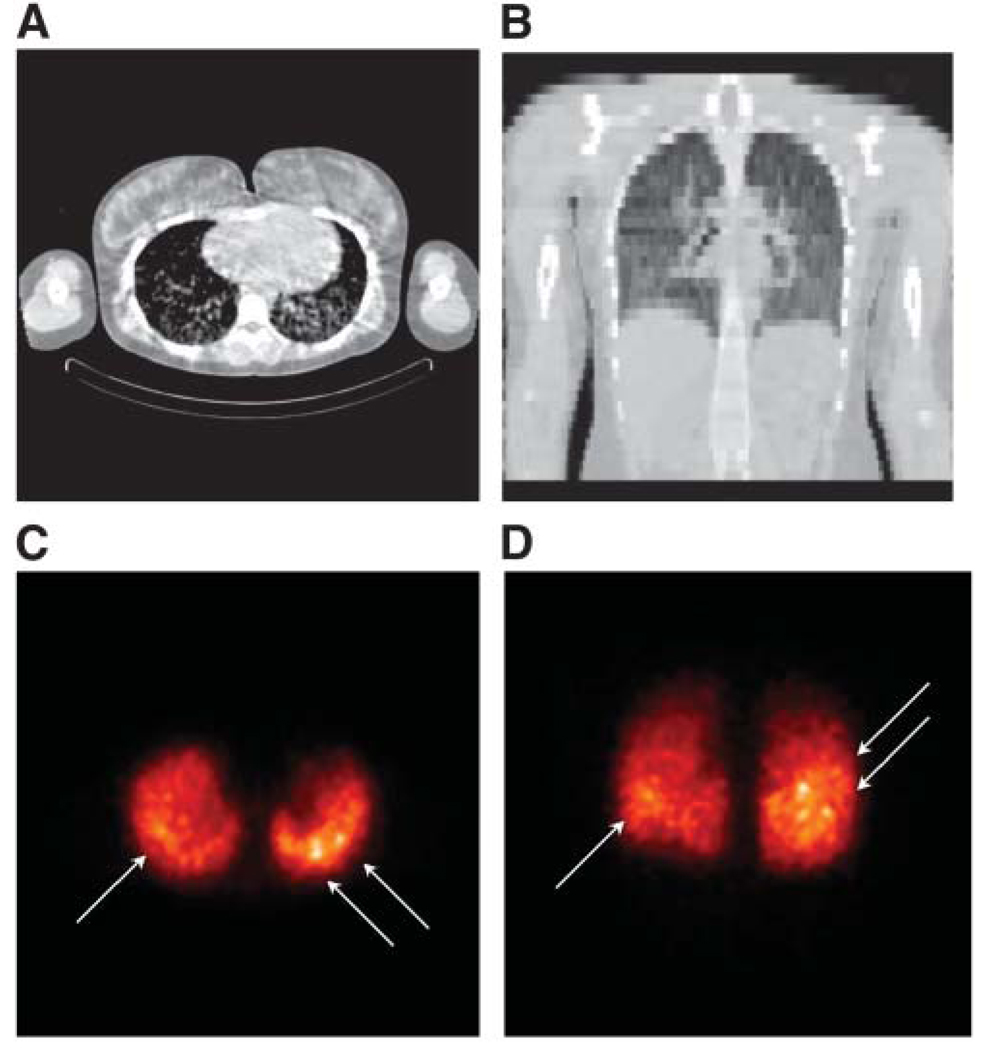
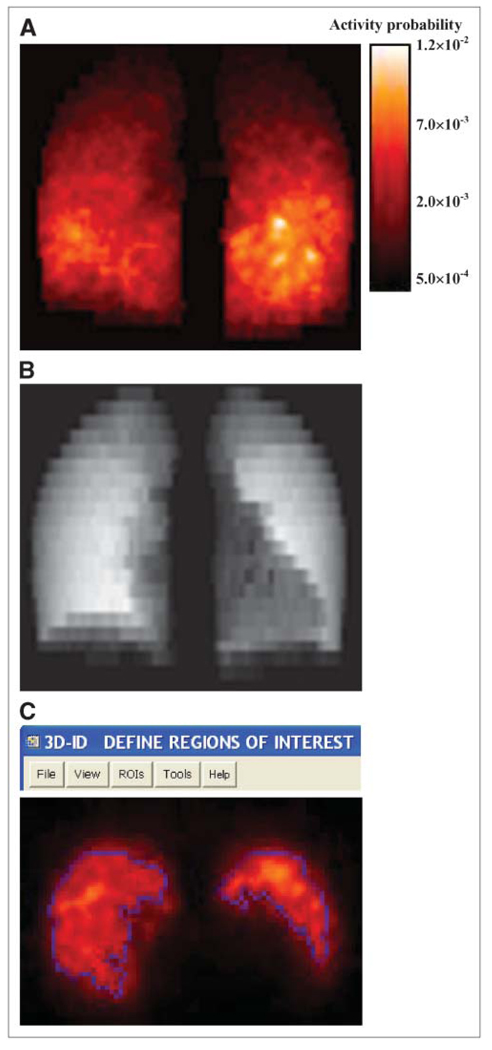
Methods: A pediatric thyroid cancer patient with diffuse lung metastases was administered 37 MBq of (131)I after preparation with rTSH. SPECT/CT scans were performed over the chest at 27, 74, and 147 h after tracer administration. The time-activity curve for (131)I in the lungs was derived from the whole-body planar imaging and compared with that obtained from the quantitative SPECT methods. Reconstructed and coregistered SPECT/CT images were converted into 3D density and activity probability maps suitable for MCNP4b input. Absorbed dose maps were calculated using electron and photon transport in MCNP4b. Administered activity was estimated on the basis of the maximum tolerated dose (MTD) of 27.25 Gy to the normal lungs. Computational efficiency of the MCNP4b code was studied with a simple segmentation approach. In addition, the Benua-Leeper method was used to estimate the recommended administered activity. The standard dosing plan was modified to account for the weight of this pediatric patient, where the 2.96-GBq (80 mCi) whole-body retention was scaled to 2.44 GBq (66 mCi) to give the same dose rate of 43.6 rad/h in the lungs at 48 h.
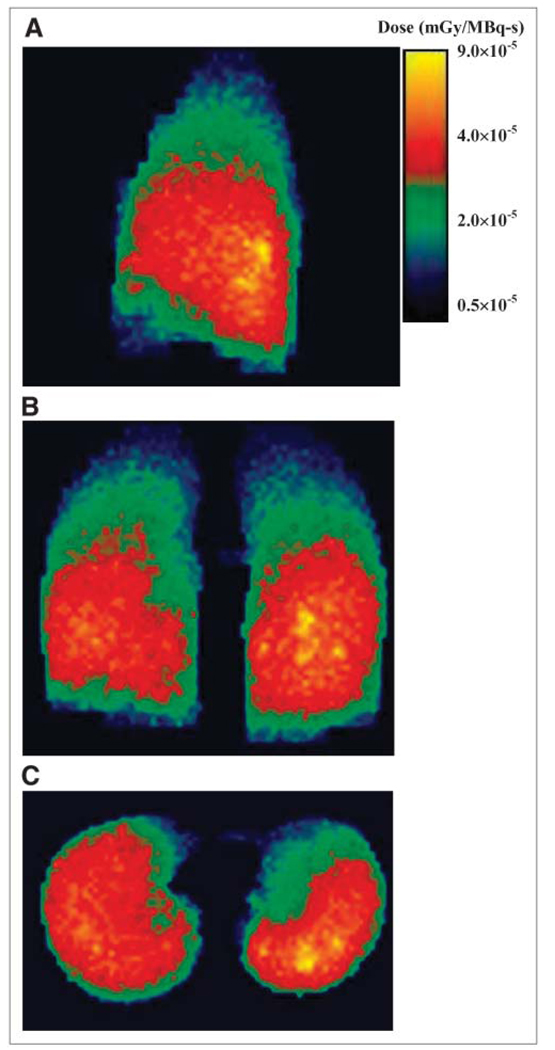
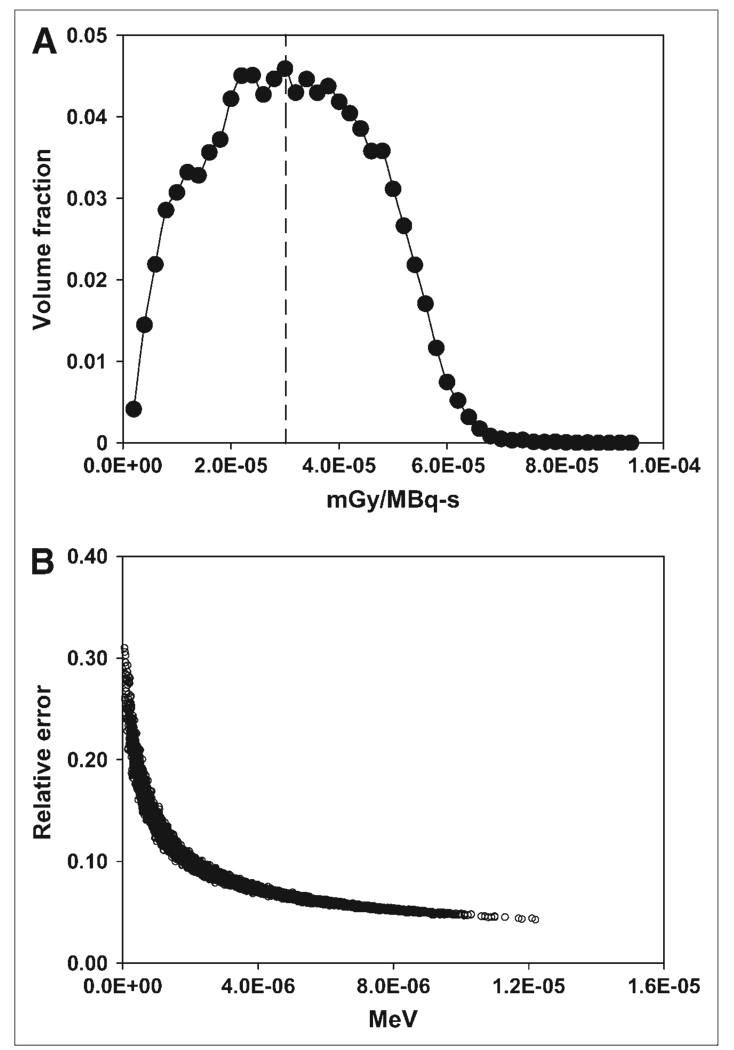
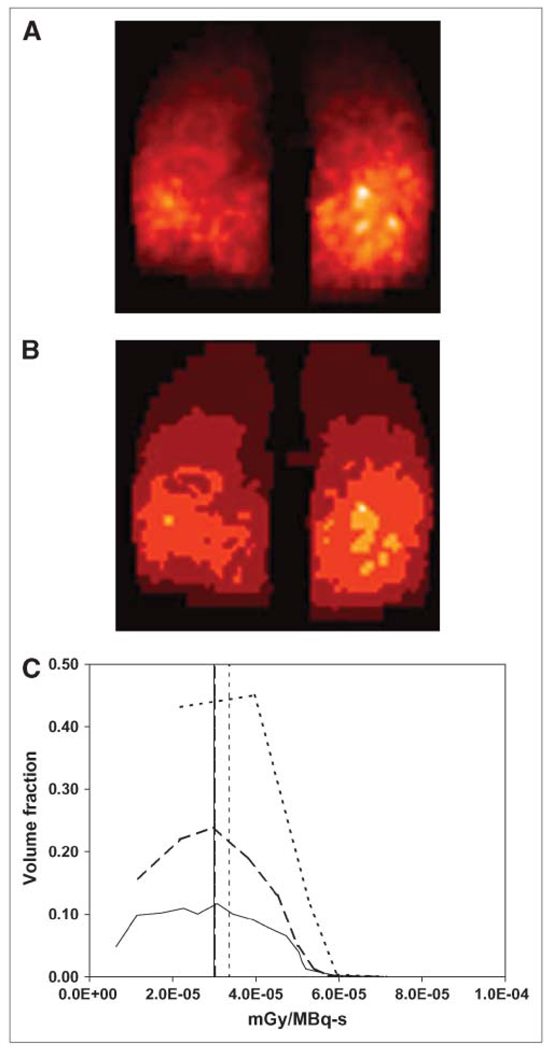
Results: Using the MCNP4b code, both the spatial dose distribution and a dose-volume histogram were obtained for the lungs. An administered activity of 1.72 GBq (46.4 mCi) delivered the putative MTD of 27.25 Gy to the lungs with a tumor absorbed dose of 63.7 Gy. Directly applying the Benua-Leeper method, an administered activity of 3.89 GBq (105.0 mCi) was obtained, resulting in tumor and lung absorbed doses of 144.2 and 61.6 Gy, respectively, when the MCNP-based dosimetry was applied. The voxel-by-voxel calculation time of 4,642.3 h for photon transport was reduced to 16.8 h when the activity maps were segmented into 20 regions.
Conclusion: MCNP4b-based, patient-specific 3D dosimetry is feasible and important in the dosimetry of thyroid cancer patients with avid lung metastases that exhibit prolonged retention in the lungs.
Figures
References
-
- Lin JD, Chao TC, Chou SC, Hsueh C. Papillary thyroid carcinomas with lung metastases. Thyroid. 2004;14:1091–1096. - PubMed
-
- Clark JR, Lai P, Hall F, Borglund A, Eski S, Freeman JL. Variables predicting distant metastases in thyroid cancer. Laryngoscope. 2005;115:661–667. - PubMed
-
- Mazzaferri EL, Kloos RT. Current approaches to primary therapy for papillary and follicular thyroid cancer. J Clin Endocrinol Metab. 2001;86:1447–1463. - PubMed
-
- Benua RS, Cicale NR, Sonerberg M, Rawson RW. The relation of radioiodine dosimetry to results and complications in the treatment of metastatic thyroid cancer. AJR. 1962;87:171–182. - PubMed
-
- Benua RS, Leeper RD. A method and rationale for treating metastatic thyroid carcinoma with the largest safe dose of 131I. In: Medeiros-Neta G, Gaitan E, editors. Frontiers in Thyroidology. New York, NY: Plenum Medical; 1986. pp. 1317–1321.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical