

Survey on the impact of comorbid allergic rhinitis in patients with asthma
- PMID: 17140421
- PMCID: PMC1698496
- DOI: 10.1186/1471-2466-6-S1-S3
Survey on the impact of comorbid allergic rhinitis in patients with asthma
Abstract
Background: Allergic rhinitis (AR) and asthma are inflammatory conditions of the airways that often occur concomitantly. This global survey was undertaken to understand patient perspectives regarding symptoms, treatments, and the impact on their well-being of comorbid AR and asthma.
Methods: Survey participants were adults with asthma (n = 813) and parents of children with asthma (n = 806) from four countries each in the Asia-Pacific region and Europe. Patients included in the survey also had self-reported, concomitant AR symptoms. Patients and parents were recruited by telephone interview or by direct interview.
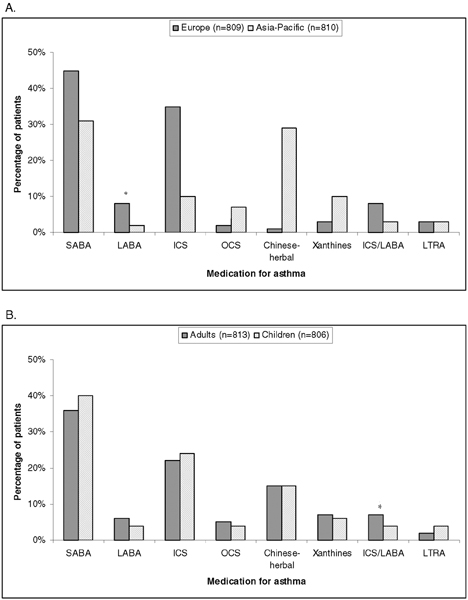
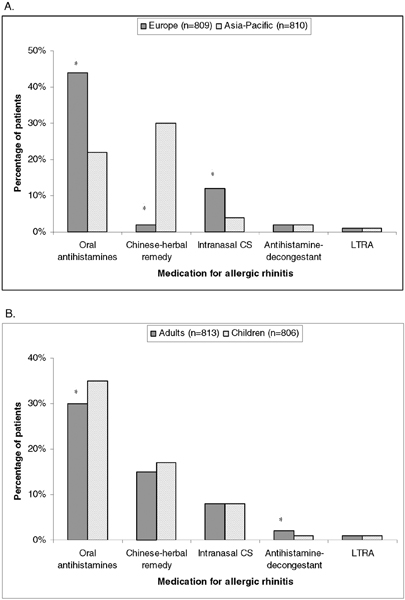
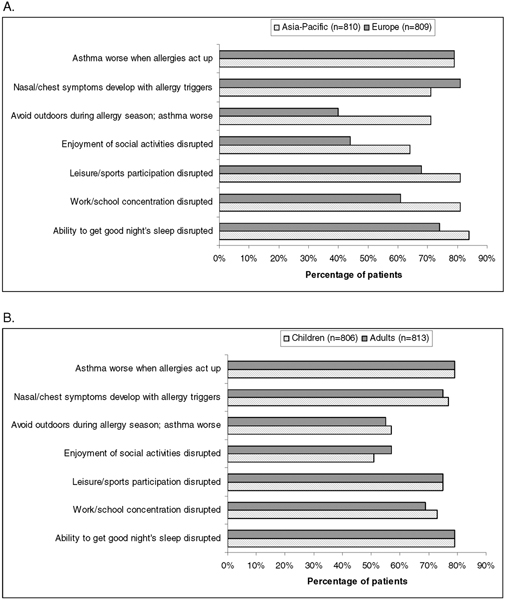
Results: Most patients (73%) had pre-existing symptoms of AR when their asthma was first diagnosed. Shortness of breath (21%) was the most troublesome symptom for adults, and wheezing (17%) and coughing (17%) the most troublesome for children. Patients used different medications for treating asthma (most commonly short-acting beta-agonists and inhaled corticosteroids) and for treating AR (most commonly oral antihistamines). The concomitant presence of AR and asthma disrupted the ability to get a good night's sleep (79%), to participate in leisure and sports activities (75%), to concentrate at work or school (69% of adults, 73% of children), and to enjoy social activities (57% of adults, 51% of children). Most patients (79%) reported worsening asthma symptoms when AR symptoms flared up. Many (56%) avoided the outdoors during the allergy season because of worsening asthma symptoms. Many (60%) indicated difficulty in effectively treating both conditions, and 72% were concerned about using excessive medication. In general, respondents from the Asia-Pacific region reported more disruption of activities caused by symptoms and more concerns and difficulties with medications than did those from Europe. Differences between the two regions in medication use included more common use of inhaled corticosteroids in Europe and more common use of Chinese herbal remedies in the Asia-Pacific region.
Conclusion: Results of this survey suggest that comorbid asthma and AR substantially impact patient well-being and that the worsening of AR symptoms in patients with asthma can be associated with worsening asthma symptoms. These findings underscore the need for physicians who treat patients with asthma to evaluate treatment options for improving symptoms of both AR and asthma when present concomitantly.
Figures
References
-
- National Institutes of Health NH Lung and Blood Institute . Updated report 2002. Bethesda, MD; 2002. Asthma management and prevention. Global Initiative for Asthma. A practical guide for public health officials and health care professionals. Based on the global strategy for asthma management and prevention NHLBI/WHO workshop report.
-
- Gaugris S, Sazonov-Kocevar V, Thomas M. Burden of concomitant allergic rhinitis in adults with asthma. J Asthma. 2006;43:1–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
