

Podokinetic after-rotation in Parkinson disease
- PMID: 17140549
- PMCID: PMC1828875
- DOI: 10.1016/j.brainres.2006.10.053
Podokinetic after-rotation in Parkinson disease
Abstract
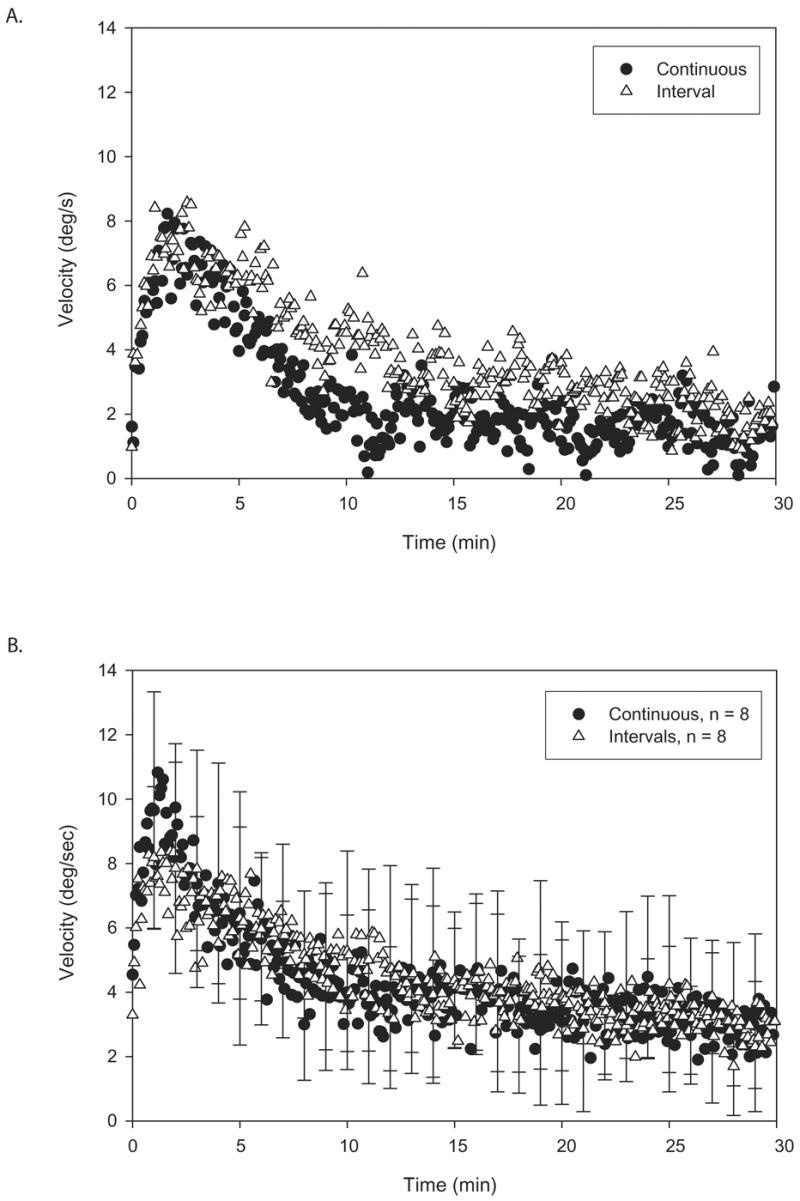
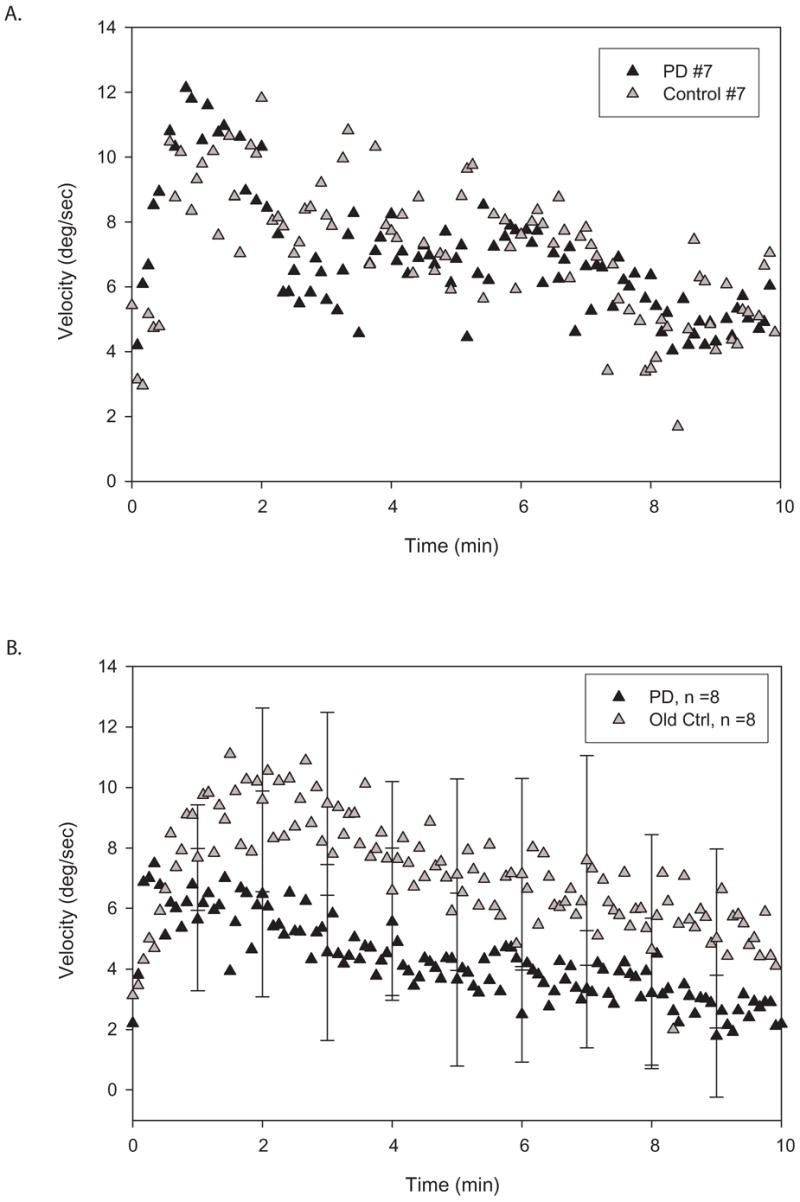
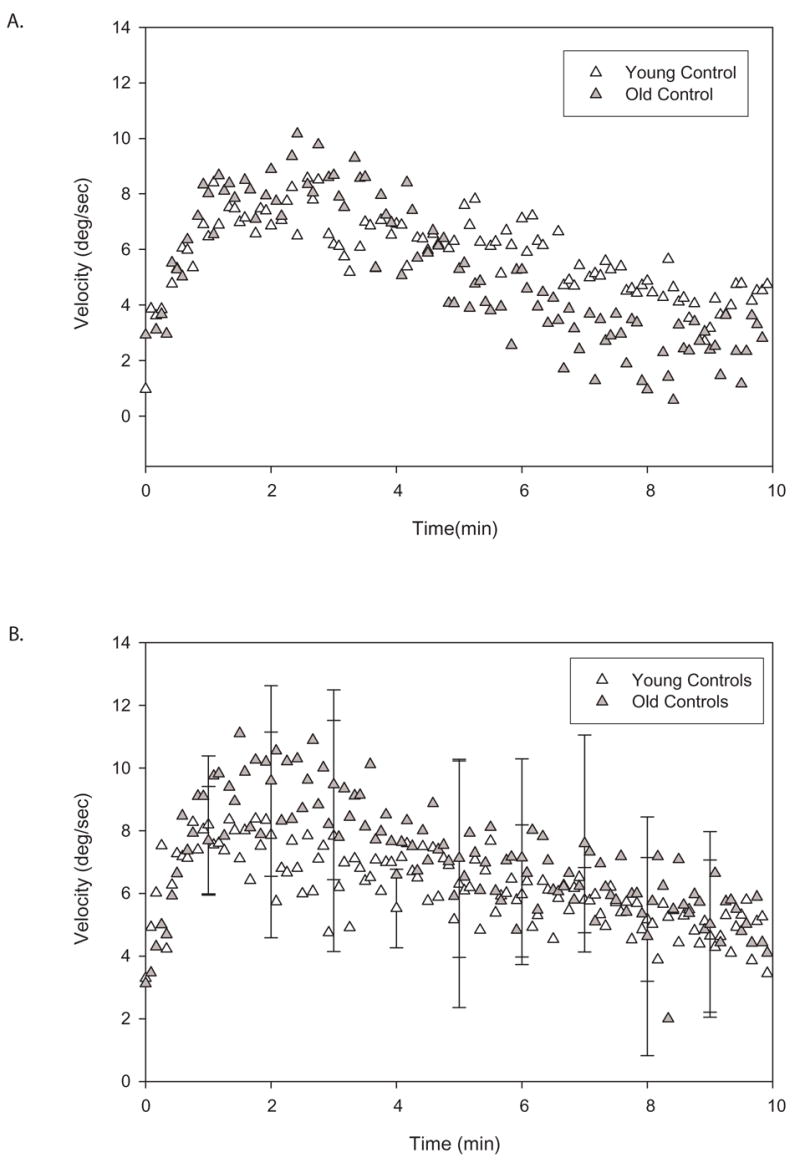
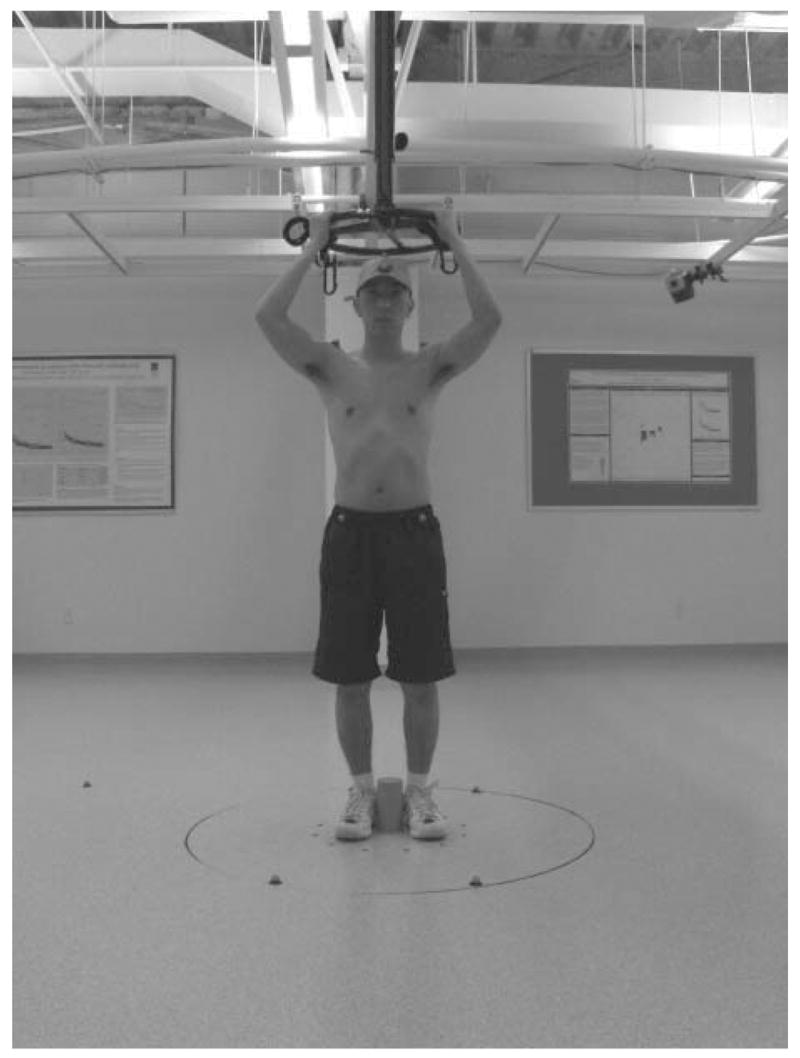
Walking on a rotating platform for 15 min causes healthy subjects to involuntarily turn when walking without vision. This adaptive response, called podokinetic after-rotation (PKAR), uses the same kinematic patterns as voluntary turning suggesting that PKAR and voluntary turning share common mechanisms. The purpose of this study is to determine whether people with Parkinson disease (PD), a condition that produces substantial disability from turning difficulties, can adapt to the rotating platform. Initial testing of people with PD revealed that most were unable to step on the rotating platform for 15 continuous minutes. We thus tested a less intense version of the paradigm in eight healthy people. On one day, subjects walked on the platform for 15 continuous minutes; on another day, they walked on the platform for three 5-minute intervals separated by 5-minute rests. After both sessions, subjects rested for 5 min then walked in place for 30 min without vision, while we recorded rotational velocity of PKAR. Continuous and interval protocols effectively elicited robust PKAR. We then tested eight subjects with PD and matched controls using the 5-minute interval protocol and recorded PKAR responses for 10 min. There were no significant differences between the PD and control groups. We conclude that PD subjects can adapt to the rotating platform and develop PKAR from interval training. Future studies are needed to determine whether the rotating platform may act as a rehabilitative tool to reinforce motor patterns for turning and alleviate turning difficulties in people with PD.
Figures
References
-
- Bagley S, Kelly B, Tunnicliffe N, Turnbull GI, Walker JM. The effect of visual cues on the gait of independently mobile Parkinson’s disease patients. Physiotherapy. 1991;77:415–420.
-
- Bloem B, Van Vugt J, Beckley D. Postural instability and falls in Parkinson’s Disease. Advances in Neurology. 2001;87:209–223. - PubMed
-
- Bloem BR, Hausdorff JM, Visser JE, Giladi N. Falls and freezing of gait in Parkinson’s disease: a review of two interconnected, episodic phenomena. Mov Disord. 2004;19(8):871–84. - PubMed
-
- Charlett A, Weller C, Purkiss A, Dobbs S, Dobbs R. Breadth of base whilst walking: effect of ageing and parkinsonism. Age and Ageing. 1998;27:49–54. - PubMed
-
- Contreras-Vidal JL, Teulings HL, Stelmach GE, Adler CH. Adaptation to changes in vertical display gain during handwriting in Parkinson’s disease patients, elderly and young controls. Parkinsonism Relat Disord. 2002;9(2):77–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
