

Mental practice with motor imagery: evidence for motor recovery and cortical reorganization after stroke
- PMID: 17140874
- PMCID: PMC2561070
- DOI: 10.1016/j.apmr.2006.08.326
Mental practice with motor imagery: evidence for motor recovery and cortical reorganization after stroke
Abstract
Objectives: To measure the efficacy of a program combining mental and physical practice with the efficacy of a program composed of only constraint-induced movement therapy (CIMT) or only mental practice on stroke patients' levels of upper-extremity impairment and upper-extremity functional outcomes and to establish the relationship between changes in blood-oxygen-level dependent (BOLD) functional magnetic resonance imaging response during a specific motor or imagery task and improvement in motor function between intervention groups.
Design: Case series.
Setting: Licensed, 56-bed, freestanding, university-affiliated rehabilitation hospital.
Participants: Three men and 1 woman with moderate upper-limb hemiparesis after stroke were randomized.
Interventions: Two patients received mental practice and CIMT, 1 patient received only mental practice, and 1 received only CIMT.
Main outcome measures: Wolf Motor Function Test (WMFT), Motor Activity Log (MAL), Sirigu break test, Movement Imagery Questionnaire-Revised, and Vividness of Movement Imagery Questionnaire.
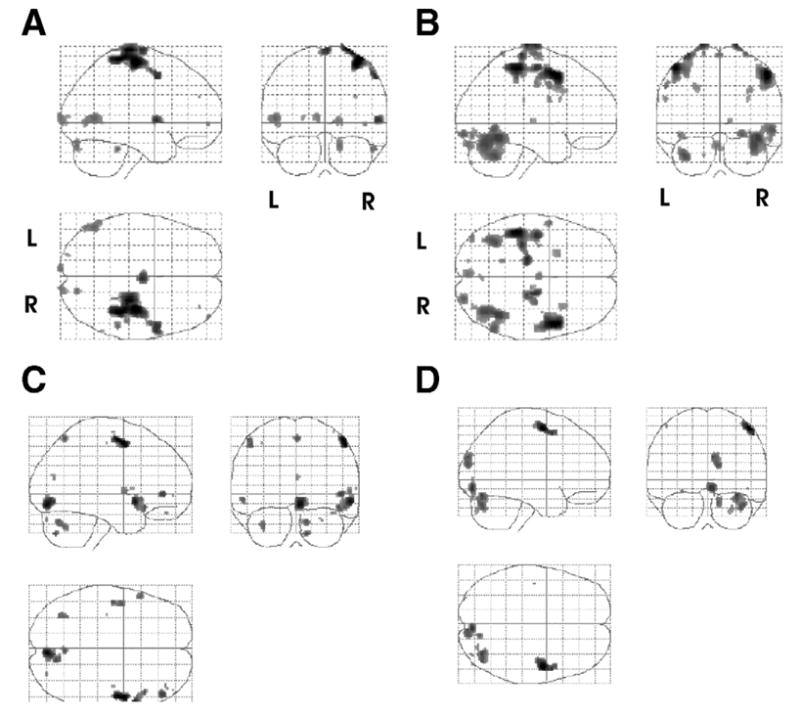
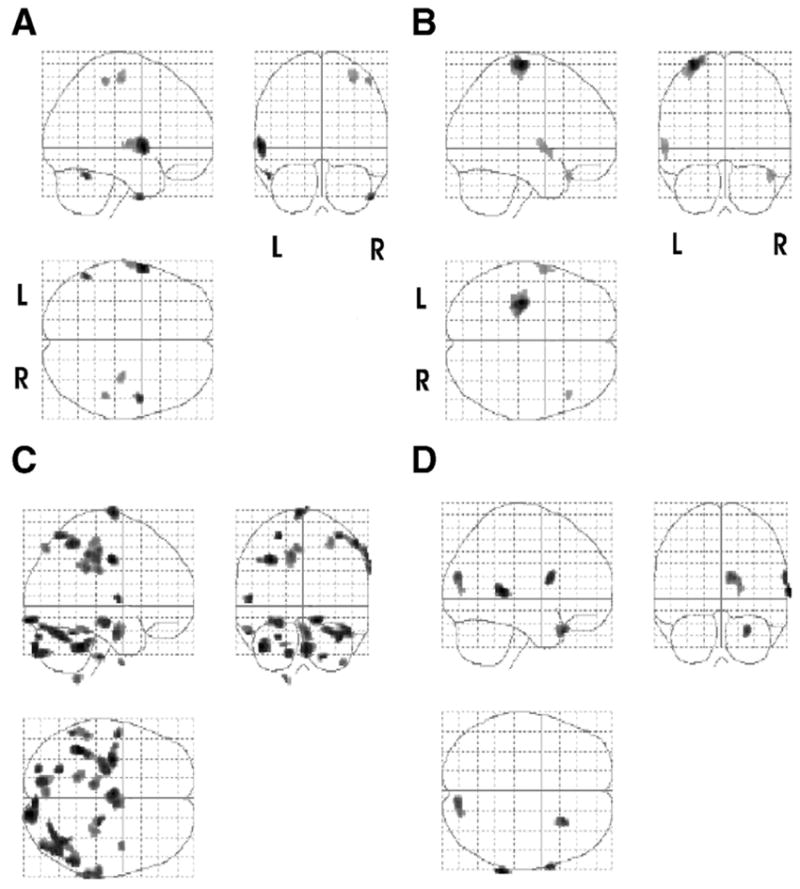
Results: The mental practice intervention alone led to slight improvement in certain functional and mental imagery measures (Sirigu, MAL, WMFT) but did not result in a clinically meaningful improvement with notable right cerebellar hemisphere activation that was not present before intervention. After CIMT, only the single patient showed clinically meaningful improvement of his affected hand as exhibited by decreased times on the MAL and WMFT. The patient showed increased bilateral cortical activation in both the motor and premotor areas during execution of a finger flexion and extension task. In contrast, during a second task, which was an imagined flexion and extension task, motor, occipital, and inferior parietal activation mainly in the contralateral hemisphere were observed. After 2 weeks of CIMT plus mental practice a patient with a lesion restricted to the parietal cortex showed little improvement in upper-extremity function and mental imagery in comparison with the patient with damage to nonparietal areas, who showed clinically meaningful improvement. The pattern of activation after 2 weeks of CIMT plus mental practice in the patient with nonparietal damage led to more focal contralateral activation in primary motor cortex when executing a voluntary flexion and extension task.
Conclusions: The case series indicates that for these patients with chronic, moderate upper-extremity impairment after stroke, a 2-week regimen of CIMT or CIMT plus mental practice only (in 1 case) resulted in modest changes occurring as a decrease in impairment, with functional improvement. Mental practice alone did not result in a clinically meaningful improvement in upper-limb impairment. We describe how these interventions may elicit "plastic" changes in the brain. Further investigations to determine the appropriate delivery and dosing of both physical and mental practice, as well as to determine whether mental practice-induced changes positively correlate with distinct patterns of cortical activation, should be undertaken before the efficacy of their use can be ascertained among patients with limitations comparable with these participants.
Figures

References
-
- Barreca S, Wolf SL, Fasoli S, Bohannon R. Treatment interventions for the paretic upper limb of stroke survivors: a critical review. Neurorehabil Neural Repair. 2003;17:220–6. - PubMed
-
- Braun SM, Beurskens AJ, Borm PJ, Schack T, Wade DT. The effects of mental practice in stroke rehabilitation: a systematic review. Arch Phys Med Rehabil. 2006;87:842–52. - PubMed
-
- Sharma N, Pomeroy VM, Baron JC. Motor imagery: a backdoor to the motor system after stroke? Stroke. 2006;37:1941–52. - PubMed
-
- Feltz D, Landers D. The effects of mental practice on motor skill learning and performance: an article. J Sport Psychol. 1983;5:25–57.
-
- Page SJ, Levine P, Sisto S, Johnston MV. A randomized efficacy and feasibility study of imagery in acute stroke. Clin Rehabil. 2001;15:233–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
