

Inpatient disposition classification for the creation of hospital surge capacity: a multiphase study
- PMID: 17141705
- PMCID: PMC7138047
- DOI: 10.1016/S0140-6736(06)69808-5
Inpatient disposition classification for the creation of hospital surge capacity: a multiphase study
Abstract
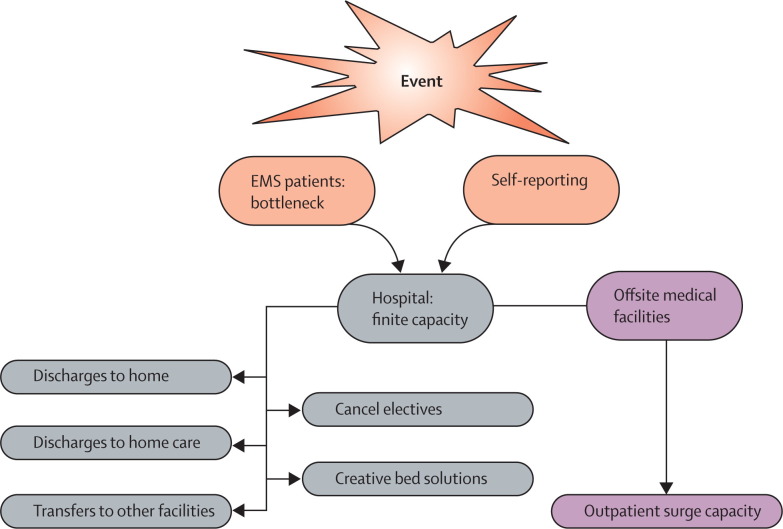
Background: The ability to provide medical care during sudden increases in patient volume during a disaster or other high-consequence event is a serious concern for health-care systems. Identification of inpatients for safe early discharge (ie, reverse triage) could create additional hospital surge capacity. We sought to develop a disposition classification system that categorises inpatients according to suitability for immediate discharge on the basis of risk tolerance for a subsequent consequential medical event.
Methods: We did a warfare analysis laboratory exercise using evidence-based techniques, combined with a consensus process of 39 expert panellists. These panellists were asked to define the categories of a disposition classification system, assign risk tolerance of a consequential medical event to each category, identify critical interventions, and rank each (using a scale of 1-10) according to the likelihood of a resultant consequential medical event if a critical intervention is withdrawn or withheld because of discharge.
Findings: The panellists unanimously agreed on a five-category disposition classification system. The upper limit of risk tolerance for a consequential medical event in the lowest risk group if discharged early was less than 4%. The next categories had upper limits of risk tolerance of about 12% (IQR 8-15%), 33% (25-50%), 60% (45-80%) and 100% (95-100%), respectively. The expert panellists identified 28 critical interventions with a likelihood of association with a consequential medical event if withdrawn, ranging from 3 to 10 on the 10-point scale.
Interpretation: The disposition classification system allows conceptual classification of patients for suitable disposition, including those deemed safe for early discharge home during surges in demand. Clinical criteria allowing real-time categorisation of patients are awaited.
Figures
Comment in
-
Reverse triage: useful for day-to-day access block?Lancet. 2006 Dec 2;368(9551):1940-1. doi: 10.1016/S0140-6736(06)69785-7. Lancet. 2006. PMID: 17141684 No abstract available.
-
Age-proofing hospital surge capacity.Lancet. 2007 Mar 10;369(9564):822-823. doi: 10.1016/S0140-6736(07)60400-0. Lancet. 2007. PMID: 17350443 No abstract available.
References
-
- Kirschenbaum L, Keen A, O'Neill P. The experience of St Vincent's Hospital, Manhattan, on September 11, 2001: preparedness, response, and lessons learned. Crit Care Med. 2005;33(suppl):S48–S52. - PubMed
-
- Cushman JG, Pachter HL, Beaton HL. Two New York City hospitals' surgical response to the September 11, 2001, terrorist attack in New York City. J Trauma. 2003;54:147–155. - PubMed
-
- Hogan DE, Waeckerle JF, Dire DJ, Lillibridge SR. Emergency department impact of the Oklahoma City terrorist bombing. Ann Emerg Med. 1999;34:160–167. - PubMed
-
- Booth CM, Stewart TE. Severe acute respiratory syndrome and critical medicine: the Toronto experience. Crit Care Med. 2005;33(suppl):S53–S60. - PubMed
-
- May AK, McGwin G, Lancaster LJ. The April 8, 1998 tornado: assessment of the trauma system response and the resulting injuries. J Trauma. 2000;48:666–672. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
