

Genetic causes of familial hypercholesterolaemia in patients in the UK: relation to plasma lipid levels and coronary heart disease risk
- PMID: 17142622
- PMCID: PMC2563208
- DOI: 10.1136/jmg.2006.038356
Genetic causes of familial hypercholesterolaemia in patients in the UK: relation to plasma lipid levels and coronary heart disease risk
Erratum in
- J Med Genet. 2009 Dec;46(12):861
- J Med Genet. 2010 Dec;47(12):862
Abstract
Aims: To determine the relative frequency of mutations in three different genes (low-density lipoprotein receptor (LDLR), APOB, PCSK9), and to examine their effect in development of coronary heart disease (CHD) in patients with clinically defined definite familial hypercholesterolaemia in UK.
Patients and methods: 409 patients with familial hypercholesterolaemia patients (158 with CHD) were studied. The LDLR was partially screened by single-strand conformational polymorphism (SSCP) (exons 3, 4, 6-10 and 14) and by using a commercial kit for gross deletions or rearrangements. APOB (p.R3500Q) and PCSK9 (p.D374Y) were detected by specific assays. Coding exons of PCSK9 were screened by SSCP.
Results: Mutations were detected in 253 (61.9%)
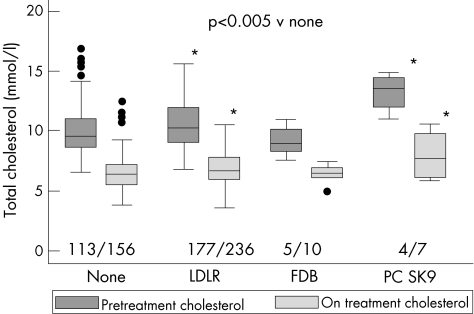
Patients: 236 (57.7%) carried LDLR, 10 (2.4%) carried APOB p.Q3500 and 7 (1.7%) PCSK9 p.Y374. No additional mutations were identified in PCSK9. After adjusting for age, sex, smoking and systolic blood pressure, compared to those with no detectable mutation, the odds ratio of having CHD in those with an LDLR mutation was 1.84 (95% CI 1.10 to 3.06), for APOB 3.40 (0.71 to 16.36), and for PCSK9 19.96 (1.88 to 211.5; p = 0.001 overall). The high risk in patients carrying LDLR and PCSK9 p.Y374 was partly explained by their higher pretreatment cholesterol levels (LDLR, PCSK9 and no mutation, 10.29 (1.85), 13.12 and 9.85 (1.90) mmol/l, respectively, p = 0.001). The post-statin treatment lipid profile in PCSK9 p.Y374 carriers was worse than in patients with no identified mutation (LDL-C, 6.77 (1.82) mmol/l v 4.19 (1.26) mmol/l, p = 0.001, HDL-C 1.09 (0.27) mmol/l v 1.36 (0.36) mmol/l, p = 0.03).
Conclusions: The higher CHD risk in patients carrying PCSK9 p.Y347 or a detected LDLR mutation supports the usefulness of DNA testing in the diagnosis and management of patients with familial hypercholesterolaemia. Mutations in PCSK9 appear uncommon in patients with familial hypercholesterolaemia in UK.
Conflict of interest statement
Competing interests: None declared.

References
-
- Slack J. Risks of ischaemic heart‐disease in familial hyperlipoproteinaemic states. Lancet 196921380–1382. - PubMed
-
- Betteridge D J, Broome K, Durrington P N, Hawkins M M, Humphries S E, Mann J I, Miller J P, Neil H A W, Thompson G R, Thorogood M, Scientific Steering Committee on behalf of the Simon Broome Register Group Mortality in treated heterozygous familial hypercholesterolaemia: implications for clinical management. Atherosclerosis 1999142105–112. - PubMed
-
- Umans‐Eckenhausen M A, Defesche J C, Sijbrands E J, Scheerder R L, Kastelein J J. Review of first 5 years of screening for familial hypercholesterolaemia in the Netherlands. Lancet 2001357165–168. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous