

Physicians' communication with patients about adherence to HIV medication in San Francisco and Copenhagen: a qualitative study using Grounded Theory
- PMID: 17144910
- PMCID: PMC1702356
- DOI: 10.1186/1472-6963-6-154
Physicians' communication with patients about adherence to HIV medication in San Francisco and Copenhagen: a qualitative study using Grounded Theory
Abstract
Background: Poor adherence is the main barrier to the effectiveness of HIV medication. The objective of this study was to explore and conceptualize patterns and difficulties in physicians' work with patients' adherence to HIV medication. No previous studies on this subject have directly observed physicians' behavior.
Methods: This is a qualitative, cross-sectional study. We used a Grounded Theory approach to let the main issues in physicians' work with patients' adherence emerge without preconceiving the focus of the study. We included physicians from HIV clinics in San Francisco, U.S.A. as well as from Copenhagen, Denmark. Physicians were observed during their clinical work and subsequently interviewed with a semi-structured interview guide. Notes on observations and transcribed interviews were analyzed with NVivo software.
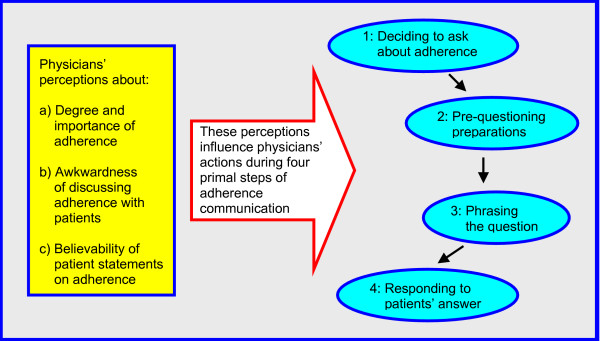
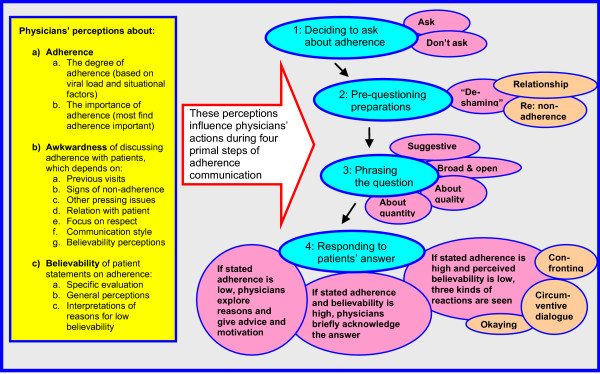
Results: We enrolled 16 physicians from San Francisco and 18 from Copenhagen. When we discovered that physicians and patients seldom discussed adherence issues in depth, we made adherence communication and its barriers the focus of the study. The main patterns in physicians' communication with patients about adherence were similar in both settings. An important barrier to in-depth adherence communication was that some physicians felt it was awkward to explore the possibility of non-adherence if there were no objective signs of treatment failure, because patients could feel "accused." To overcome this awkwardness, some physicians consciously tried to "de-shame" patients regarding non-adherence. However, a recurring theme was that physicians often suspected non-adherence even when patients did not admit to have missed any doses, and physicians had difficulties handling this low believability of patient statements. We here develop a simple four-step, three-factor model of physicians' adherence communication. The four steps are: deciding whether to ask about adherence or not, pre-questioning preparations, phrasing the question, and responding to the patient's answer. The three factors/determinants are: physicians' perceptions of adherence, awkwardness, and believability.
Conclusion: Communication difficulties were a main barrier in physicians' work with patients' adherence to HIV medication. The proposed model of physicians' communication with patients about adherence--and the identification of awkwardness and believability as key issues--may aid thinking on the subject for use in clinical practice and future research.
Figures
Similar articles
-
Physician beliefs about antiretroviral adherence communication.AIDS Patient Care STDS. 2000 Sep;14(9):477-84. doi: 10.1089/108729100438854. AIDS Patient Care STDS. 2000. PMID: 11051630
-
Adherence communication: a qualitative analysis of physician-patient dialogue.AIDS. 1999 Sep 10;13(13):1771-8. doi: 10.1097/00002030-199909100-00022. AIDS. 1999. PMID: 10509580
-
A qualitative study examining HIV antiretroviral adherence counseling and support in community pharmacies.J Manag Care Pharm. 2013 Jul-Aug;19(6):454-60. doi: 10.18553/jmcp.2013.19.6.454. J Manag Care Pharm. 2013. PMID: 23806059 Free PMC article.
-
Physician contributions to disparities in HIV/AIDS care: the role of provider perceptions regarding adherence.Curr HIV/AIDS Rep. 2005 Nov;2(4):189-93. doi: 10.1007/s11904-005-0015-5. Curr HIV/AIDS Rep. 2005. PMID: 16343377 Review.
-
Health Care Provider Barriers to HIV Pre-Exposure Prophylaxis in the United States: A Systematic Review.AIDS Patient Care STDS. 2020 Mar;34(3):111-123. doi: 10.1089/apc.2019.0189. Epub 2020 Feb 28. AIDS Patient Care STDS. 2020. PMID: 32109141 Free PMC article.
Cited by
-
Urine tenofovir testing for real-time PrEP adherence feedback: a qualitative study involving transgender women in Uganda.J Int AIDS Soc. 2024 May;27(5):e26255. doi: 10.1002/jia2.26255. J Int AIDS Soc. 2024. PMID: 38695107 Free PMC article. Clinical Trial.
-
Does the Quality of Behavior Change Counseling in Routine HIV Care Vary According to Topic and Demand?AIDS Behav. 2023 Nov;27(11):3780-3788. doi: 10.1007/s10461-023-04135-8. Epub 2023 Oct 4. AIDS Behav. 2023. PMID: 37792233
-
Establishing Novel Antiretroviral Imaging for Hair to Elucidate Nonadherence: Protocol for a Single-Arm Cross-sectional Study.JMIR Res Protoc. 2023 Apr 21;12:e41188. doi: 10.2196/41188. JMIR Res Protoc. 2023. PMID: 37083754 Free PMC article.
-
Disparity in physician perception of patients' adherence to medications by obesity status.Obesity (Silver Spring). 2010 Oct;18(10):1932-7. doi: 10.1038/oby.2010.35. Epub 2010 Feb 25. Obesity (Silver Spring). 2010. PMID: 20186132 Free PMC article.
-
Pharmacist counseling in a cohort of women with HIV and women at risk for HIV.Patient Prefer Adherence. 2012;6:457-63. doi: 10.2147/PPA.S30797. Epub 2012 Jun 18. Patient Prefer Adherence. 2012. PMID: 22791983 Free PMC article.
References
-
- Dybul M, Fauci AS, Bartlett JG, Kaplan JE, Pau AK. Guidelines for using antiretroviral agents among HIV-infected adults and adolescents. Ann Intern Med. 2002;137:381–433. - PubMed
-
- Barfod T, Gerstoft J, Rodkjær L, Pedersen C, Nielsen H, Møller A, Kristensen LH, Sørensen HT, Obel N. Patients' answers to simple questions about treatment satisfaction and adherence, and depression are associated with failure of HAART. A cross-sectional survey. Aids Patient Care and STD's. 2005;19:317–325. doi: 10.1089/apc.2005.19.317. - DOI - PubMed
-
- Wood E, Hogg RS, Yip B, Harrigan PR, O'Shaughnessy MV, Montaner JS. The impact of adherence on CD4 cell count responses among HIV-infected patients. JAIDS. 2004;35:261–268. - PubMed
