

Predicting prognosis and effect of antibiotic treatment in rhinosinusitis
- PMID: 17148625
- PMCID: PMC1687172
- DOI: 10.1370/afm.600
Predicting prognosis and effect of antibiotic treatment in rhinosinusitis
Abstract
Purpose: In evaluating complaints suggestive of rhinosinusitis, family physicians have to rely chiefly on the findings of a history, a physical examination, and plain radiographs. Yet, evidence of the value of signs, symptoms, or radiographs in the management of these patients is sparse. We aimed to determine whether clinical signs and symptoms or radiographic findings can predict the duration of the illness, the effect of antibiotic treatment, or both.
Methods: We analyzed data from 300 patients with rhinosinusitis-like complaints participating in a randomized controlled trial comparing amoxicillin with placebo. We used Cox regression analysis to assess the association between the presence at baseline of rhinosinusitis signs and symptoms or an abnormal radiograph and the subsequent course of the illness. We then tested for interactions to assess whether the presence of any of these findings predicted a beneficial effect of antibiotic treatment.
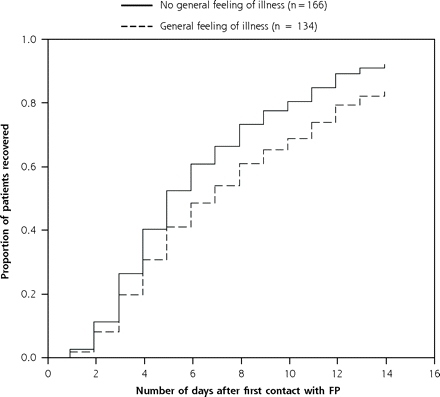
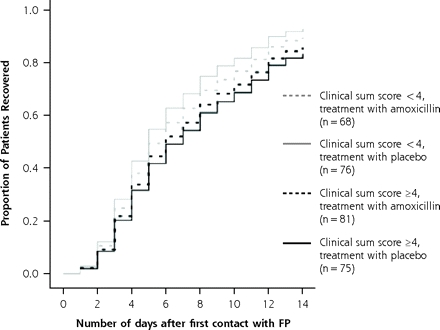
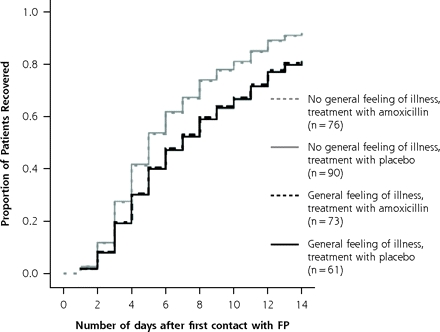
Results: Two factors at baseline were independently associated with a prolonged course of the illness: a general feeling of illness (hazard ratio = 0.77, 95% confidence interval, 0.60-0.99) and reduced productivity (hazard ratio = 0.68, 95% confidence interval, 0.53-0.88). Neither typical sinusitis signs and symptoms nor abnormal radiographs had any prognostic value. Prognosis remained unchanged whether or not patients were treated with antibiotics, no matter what symptoms patients had at baseline.
Conclusions: In a large group of average patients with rhinosinusitis, neither the presence of typical signs or symptoms nor an abnormal radiograph provided information with regard to the prognosis or the effect of amoxicillin. The time to recovery was longer in patients who felt ill at baseline or who did not feel able to work, but the course of their illness was not influenced by antibiotic treatment.
Figures

Comment in
-
A new look at an old problem: inappropriate antibiotics for acute respiratory infections.Ann Fam Med. 2006 Nov-Dec;4(6):484-5. doi: 10.1370/afm.647. Ann Fam Med. 2006. PMID: 17148624 Free PMC article. No abstract available.
References
-
- Okkes I, Oskam S, Lamberts H. Van Klacht naar Diagnose. Episodegegevens uit de Huisartspraktijk. Bussum, Netherlands: Coutinho; 1998.
-
- Gananca M, Trabulsi LR. The therapeutic effects of cyclacillin in acute sinusitis: in vitro and in vivo correlations in a placebo-controlled study. Curr Med Res Opin. 1973;1:362–368. - PubMed
-
- Wald ER, Chiponis D, Ledesma-Medina J. Comparative effectiveness of amoxicillin and amoxicillin-clavulanate potassium in acute paranasal sinus infections in children: a double-blind, placebo-controlled trial. Pediatrics. 1986;77:795–800. - PubMed
-
- Hansen JG, Schmidt H, Grinsted P. Randomised, double blind, placebo controlled trial of penicillin V in the treatment of acute maxillary sinusitis in adults in general practice. Scand J Prim Health Care. 2000;18:44–47. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical