

The American Thoracic Society's spirometric criteria alone is inadequate in asthma diagnosis
- PMID: 17149462
- PMCID: PMC2683331
- DOI: 10.1155/2006/198940
The American Thoracic Society's spirometric criteria alone is inadequate in asthma diagnosis
Abstract
Background: The diagnosis of asthma is based on clinical symptoms, physical examination and pulmonary function tests, and can be very challenging. Most patients with asthma have a significant postbronchodilator response on spirometry indicating airway hyperresponsiveness. However, having a significant bronchodilator response by itself is not diagnostic of asthma. The definition of a 'significant' response has also been controversial. Many respirologists use the American Thoracic Society (ATS) postbronchodilator response criteria of 12% (provided it is 200 mL or greater) improvement in forced expiratory volume in 1 s (or forced vital capacity) from the baseline spirometry.
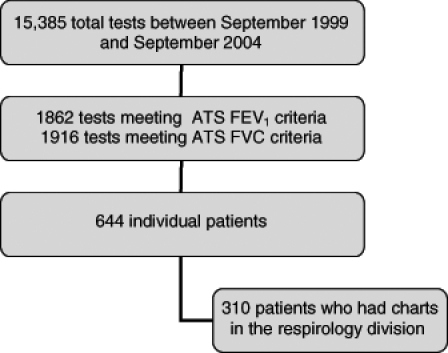
Methods: In the present study, 644 patients who met the ATS criteria for a significant postbronchodilator spirometric response were retrospectively reviewed. The staff respirologist's diagnosis of asthma, based on all clinical and pulmonary function data, was used as the standard for the diagnosis of asthma.
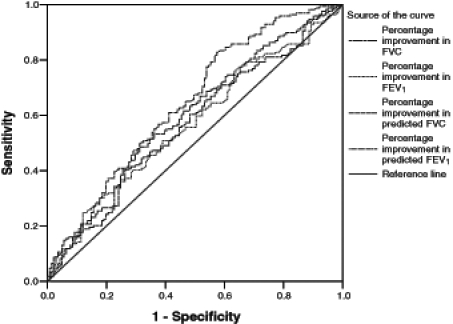
Results: Relying on spirometric criteria alone was inadequate in asthma diagnosis because only 54.7% of 310 patients who met the ATS bronchodilator response criteria were thought to have clinical asthma. Increasing the postbronchodilator percentage improvement from the ATS criteria only marginally improved diagnostic specificity and resulted in a decline in sensitivity.
Conclusions: The results of the present study further emphasize the need to use spirometric criteria as a guide but not as an unimpeachable gold standard with which to make a diagnosis of asthma. The diagnosis of asthma depends on expert physician correlation of patient history, physical examination and pulmonary function test results.
HISTORIQUE :: Le diagnostic d’asthme se fonde sur les symptômes cli-niques, l’examen physique et les explorations fonctionnelles respiratoires et peut être très complexe. La plupart des patients asthmatiques ont une réponse importante à la spirométrie après l’administration d’un bron-chodilatateur, indicatrice d’une hyperréactivité. Cependant, une réponse importante à l’administration d’un bronchodilatateur ne constitue pas en soi un diagnostic d’asthme. D’ailleurs, la définition de réponse « importante » est controversée. De nombreux pneumologues utilisent les critères d’amélioration du volume expiratoire maximal par seconde (capacité vitale forcée) de 12 % après l’administration d’un bronchodilatateur (pourvu qu’elle soit d’au moins 200 mL) par rapport à la spirométrie de base.
MÉTHODOLOGIE :: Dans la présente étude, 644 patients qui respectaient les critères de réponse importante à la spirométrie après l’administration d’un bronchodilatateur établis par l’ATS ont fait l’objet d’une analyse rétrospective. Le diagnostic d’asthme posé par le pneumologue traitant d’après toutes les données relatives à la fonction clinique et pulmonaire, a été utilisé comme norme pour le diagnostic d’asthme.
RÉSULTATS :: On ne pouvait se fier seulement aux critères spirométriques pour poser un diagnostic d’asthme, parce qu’on pensait que seulement 54,7 % des 310 patients qui respectaient les critères de réponse de l’ATS après l’administration d’un bronchodilatateur étaient atteints d’asthme clinique. Le fait d’accroître le pourcentage d’amélioration après l’administration d’un bronchodilatateur selon les critères de l’ATS n’améliorait que légèrement la spécificité diagnostique et entraînait une diminution de la sensibilité.
CONCLUSIONS :: Les résultats de la présente étude font ressortir davantage la nécessité d’utiliser les critères spirométriques pour orienter le diagnostic, qui ne constituent toutefois pas la norme d’excellence irrécusable pour poser un diagnostic d’asthme. Le diagnostic d’asthme dépend de la corrélation, déterminée par un médecin expert, avec les antécédents du patient, son examen physique et les résultats de l’exploration fonctionnelle respiratoire.
Figures
Similar articles
-
Diagnostic Accuracy of Bronchodilator Response for Asthma in a Population of South China.Adv Ther. 2018 Oct;35(10):1578-1584. doi: 10.1007/s12325-018-0783-0. Epub 2018 Sep 12. Adv Ther. 2018. PMID: 30209751
-
Comparison of bronchodilator response in patients with asthma and healthy subjects using spirometry and oscillometry.Ann Allergy Asthma Immunol. 2011 Oct;107(4):317-22. doi: 10.1016/j.anai.2011.07.011. Ann Allergy Asthma Immunol. 2011. PMID: 21962091
-
The objective evaluation of obstructive pulmonary diseases with spirometry.Int J Chron Obstruct Pulmon Dis. 2016 Aug 25;11:2009-15. doi: 10.2147/COPD.S113774. eCollection 2016. Int J Chron Obstruct Pulmon Dis. 2016. PMID: 27616884 Free PMC article.
-
Interpreting spirometry: the basics.Otolaryngol Clin North Am. 2014 Feb;47(1):39-53. doi: 10.1016/j.otc.2013.10.002. Otolaryngol Clin North Am. 2014. PMID: 24286678 Review.
-
Phenotype of asthma-chronic obstructive pulmonary disease overlap syndrome.Korean J Intern Med. 2015 Jul;30(4):443-9. doi: 10.3904/kjim.2015.30.4.443. Epub 2015 Jun 29. Korean J Intern Med. 2015. PMID: 26161009 Free PMC article. Review.
Cited by
-
Diagnosis of asthma in adults.CMAJ. 2009 Nov 10;181(10):E210-20. doi: 10.1503/cmaj.080006. Epub 2009 Sep 21. CMAJ. 2009. PMID: 19770241 Free PMC article. Review. No abstract available.
-
A Pragmatic Primary Practice Approach to Using Specific IgE in Allergy Testing in Asthma Diagnosis, Management, and Referral.J Asthma Allergy. 2022 Aug 16;15:1069-1080. doi: 10.2147/JAA.S362588. eCollection 2022. J Asthma Allergy. 2022. PMID: 35996427 Free PMC article. Review.
-
Aeroallergen sensitization for detecting asthma in primary care: A diagnostic test accuracy study.Clin Exp Allergy. 2021 Aug;51(8):1080-1084. doi: 10.1111/cea.13888. Epub 2021 May 11. Clin Exp Allergy. 2021. PMID: 33914988 Free PMC article. No abstract available.
-
An estimate of asthma prevalence in Africa: a systematic analysis.Croat Med J. 2013 Dec;54(6):519-31. doi: 10.3325/cmj.2013.54.519. Croat Med J. 2013. PMID: 24382846 Free PMC article.
-
Novel approach to continuous adventitious respiratory sound analysis for the assessment of bronchodilator response.PLoS One. 2017 Feb 8;12(2):e0171455. doi: 10.1371/journal.pone.0171455. eCollection 2017. PLoS One. 2017. PMID: 28178317 Free PMC article.
References
-
- National Asthma Education and Prevention Program. Expert panel report 2: Guidelines for the diagnosis and management of asthma. <http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf> (Version current at September 25, 2006).
-
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS, GOLD Scientific Committee Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163:1256–76. - PubMed
-
- Pellegrino R, Rodarte JR, Brusasco V. Assessing the reversibility of airway obstruction. Chest. 1998;114:1607–12. - PubMed
-
- Anthonisen NR, Wright EC. Bronchodilator response in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1986;133:814–9. - PubMed
-
- Eliasson O, Degraff AC., Jr The use of criteria for reversibility and obstruction to define patient groups for bronchodilator trials. Influence of clinical diagnosis, spirometric, and anthropometric variables. Am Rev Respir Dis. 1985;132:858–64. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
