

Prediction of valve prosthesis-patient mismatch prior to aortic valve replacement: which is the best method?
- PMID: 17164480
- PMCID: PMC1955566
- DOI: 10.1136/hrt.2006.102764
Prediction of valve prosthesis-patient mismatch prior to aortic valve replacement: which is the best method?
Abstract
Background: To predict the occurrence of valve prosthesis-patient mismatch (VP-PM) after aortic valve replacement (AVR), the surgeon needs to estimate the postoperative effective orifice area index (EOAI).
Aim: To compare different methods of predicting VP-PM.
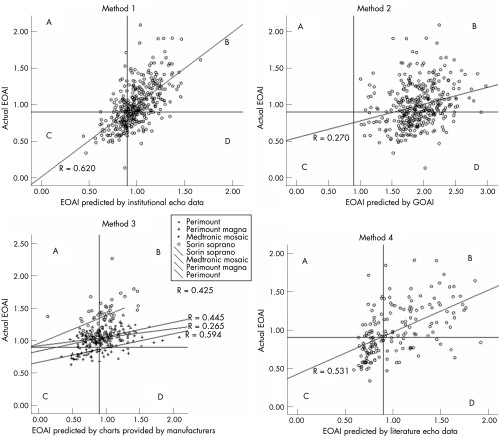
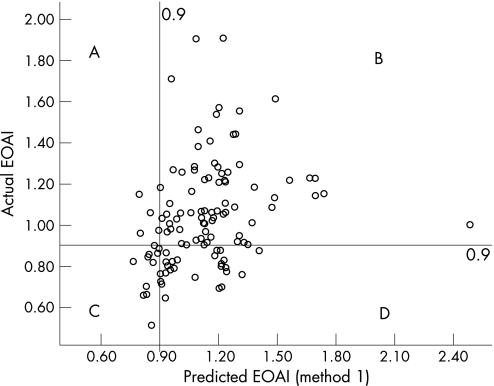
Methods: The effective orifice area (EOA) of 383 patients who had undergone AVR between July 2000 and January 2005 with various aortic valve prostheses was obtained echocardiographically 6 months after the operation. We tested the efficacy of (1) EOAI calculated from the echo data obtained in our own laboratory, (2) indexed geometric orifice area, (3) EOAI estimated from charts provided by prosthesis manufacturers (which are based either on in vitro or on echo data) and (4) EOAI estimated from reference echo data published in the literature to predict VP-PM.
Results: Sensitivity and specificity to predict VP-PM were 53% and 83% (method 1), 80% and 53% (charts based on echo data, parts of method 3) and 71% and 67% (method 4) using reference data derived from echocardiographic examinations. The sensitivity of method 2 and of charts based on in vitro data (parts of method 3) to predict VP-PM was 0-17%. The incidence of severe VP-PM could be reduced from 8.7% to 0.8% after the introduction of the systematic estimation of the EOAI at the time of operation (p = 0.003, method 1).
Conclusions: The best method of predicting VP-PM is the use of mean (SD) EOAs derived from echocardiographic examinations, whereas the use of in vitro data or the geometric orifice area is unreliable. After the surgeon's anticipation of VP-PM prior to AVR, the incidence of VP-PM could be reduced.
Conflict of interest statement
Competing interests: None.
Comment in
-
Prevention of valve prosthesis--patient mismatch before aortic valve replacement: does it matter and is it feasible?Heart. 2007 May;93(5):549-51. doi: 10.1136/hrt.2006.107672. Heart. 2007. PMID: 17435068 Free PMC article.
References
-
- Rahimtoola S H. The problem of valve prosthesis‐patient mismatch. Circulation 19785820–24. - PubMed
-
- Pibarot P, Dumesnil J G, Lemieux M.et al Impact of prosthesis‐patient mismatch on hemodynamic and symptomatic status, morbidity and mortality after aortic valve replacement with a bioprosthetic heart valve. J Heart Valve Dis 19987211–218. - PubMed
-
- Blais C, Dumesnil J G, Baillot R.et al Impact of valve prosthesis‐patient mismatch on short‐term mortality after aortic valve replacement. Circulation 2003108983–988. - PubMed
-
- Tasca G, Mhagna Z, Perotti S.et al Impact of prosthesis‐patient mismatch on cardiac events and midterm mortality after aortic valve replacement in patients with pure aortic stenosis, Circulation 2006113570–576. - PubMed
-
- Mohty‐Echahidi D, Malouf J F, Girard S E.et al Impact of prosthesis‐patient mismatch on long‐term survival in patients with small St Jude Medical mechanical prostheses in the aortic position. Circulation 2006113420–426. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources