

Systematic review on the recurrence of postoperative nausea and vomiting after a first episode in the recovery room - implications for the treatment of PONV and related clinical trials
- PMID: 17166262
- PMCID: PMC1712223
- DOI: 10.1186/1471-2253-6-14
Systematic review on the recurrence of postoperative nausea and vomiting after a first episode in the recovery room - implications for the treatment of PONV and related clinical trials
Abstract
Background: Despite the presence of a plethora of publications on the prevention of postoperative nausea and vomiting (PONV) only little is known how to treat established symptoms. Besides the high effort of performing these efficacy trials (much more patients must give their consent than are actually included in a study) and ethical concerns, little is known about the rate of re-occurring PONV/vomiting after placebo. As a consequence investigators will have difficulties defining a clinically relevant effect for the new treatment which is crucial for any planning. A quantitative systematic review was performed in order to provide more reliable estimates of the incidence of re-occurring PONV/vomiting after placebo and to help investigators defining a clinically relevant treatment effect.
Methods: A systematic search of the literature was performed using an extended search strategy of a previous review. Data on the recurrence of PONV (any nausea or emetic symptom) and vomiting (retching or vomiting) was extracted from published reports treating PONV with placebo and unpublished results from two observational trials where no treatment was given. A nonlinear random effects model was used to calculate estimates of the recurrence of symptoms and their 95%-confidence intervals (95%-CI).
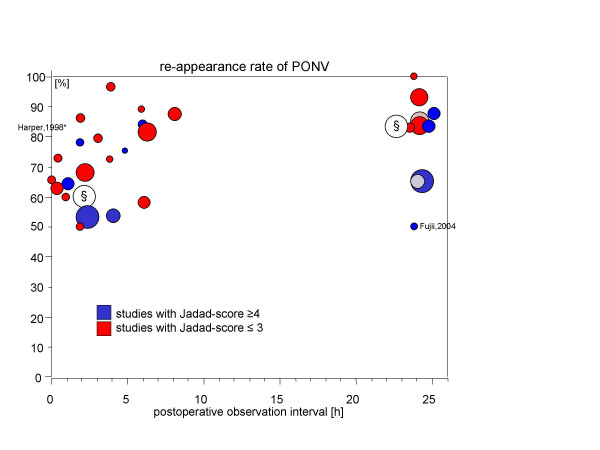
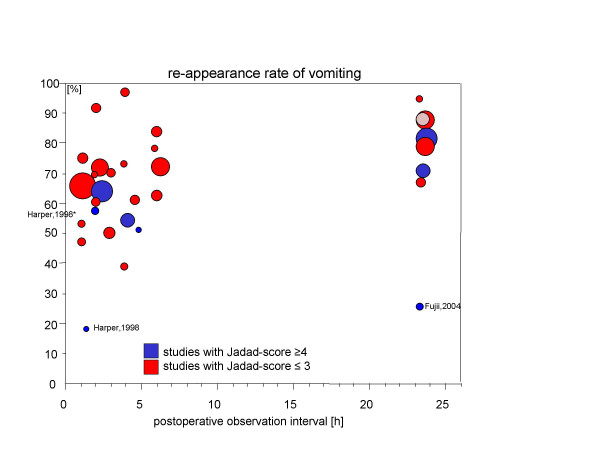
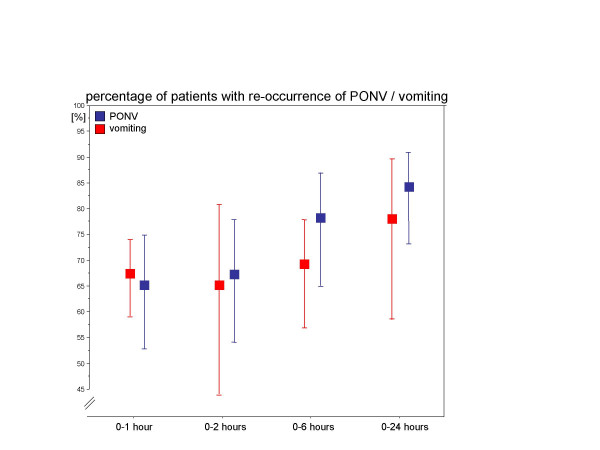
Results: A total of 29 trials (including the unpublished data) were eligible for the calculations. Depending on the length of observation after administering placebo or no treatment the recurrence rate of PONV was between 65% (95%-CI: 53%...75%) and 84% (95%-CI: 73%...91%) and that of vomiting was between 65% (95%-CI: 44%...81%) and 78% (95%-CI: 59%...90%).
Conclusion: Almost all trials showed a considerable and consistently high rate of recurrence of emetic symptoms after placebo highlighting the need for a consequent antiemetic treatment. Future (placebo) controlled efficacy trials may use the presented empirical estimates for defining clinically relevant effects and for statistical power considerations.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
