

Anthroposophic therapy for chronic depression: a four-year prospective cohort study
- PMID: 17173663
- PMCID: PMC1764730
- DOI: 10.1186/1471-244X-6-57
Anthroposophic therapy for chronic depression: a four-year prospective cohort study
Abstract
Background: Depressive disorders are common, cause considerable disability, and do not always respond to standard therapy (psychotherapy, antidepressants). Anthroposophic treatment for depression differs from ordinary treatment in the use of artistic and physical therapies and special medication. We studied clinical outcomes of anthroposophic therapy for depression.
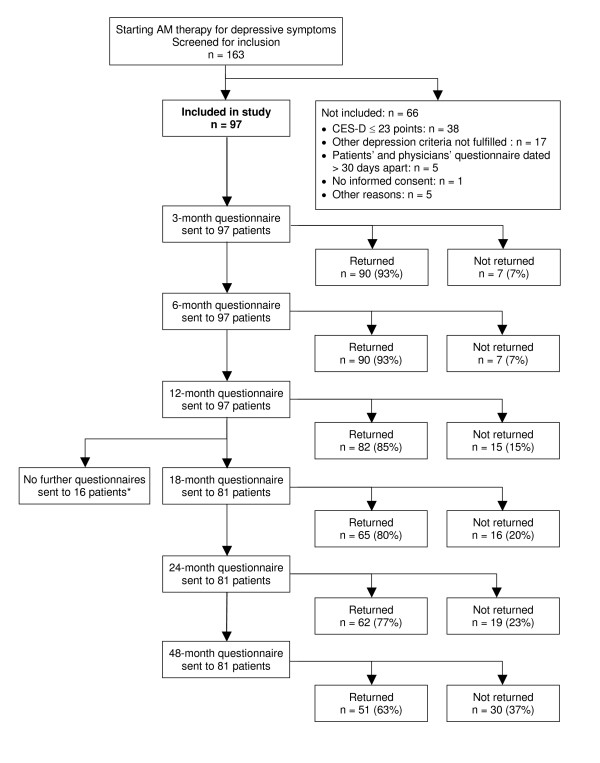
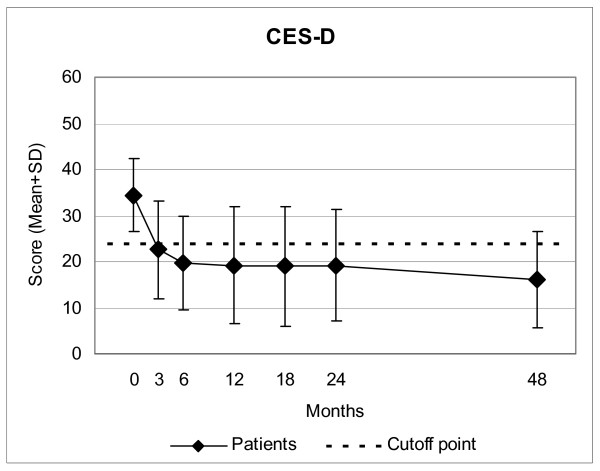
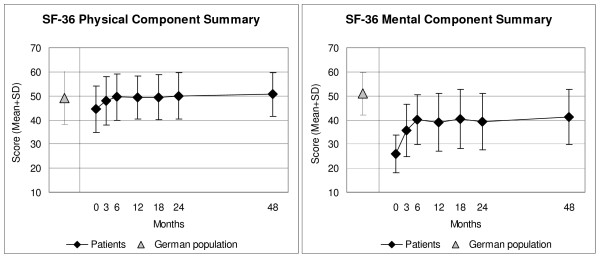
Methods: 97 outpatients from 42 medical practices in Germany participated in a prospective cohort study. Patients were aged 20-69 years and were referred to anthroposophic therapies (art, eurythmy movement exercises, or rhythmical massage) or started physician-provided anthroposophic therapy (counselling, medication) for depression: depressed mood, at least two of six further depressive symptoms, minimum duration six months, Center for Epidemiological Studies Depression Scale, German version (CES-D, range 0-60 points) of at least 24 points. Outcomes were CES-D (primary outcome) and SF-36 after 3, 6, 12, 18, 24, and 48 months. Data were collected from July 1998 to March 2005.
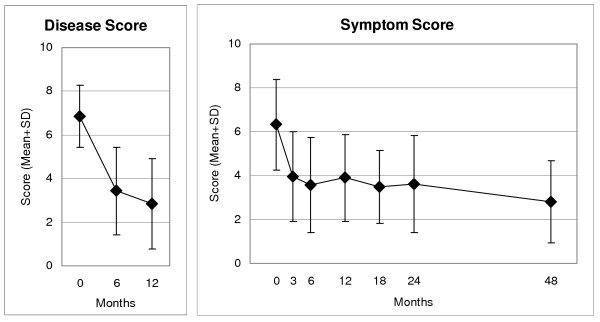
Results: Median number of art/eurythmy/massage sessions was 14 (interquartile range 12-22), median therapy duration was 137 (91-212) days. All outcomes improved significantly between baseline and all subsequent follow-ups. Improvements from baseline to 12 months were: CES-D from mean (standard deviation) 34.77 (8.21) to 19.55 (13.12) (p < 0.001), SF-36 Mental Component Summary from 26.11 (7.98) to 39.15 (12.08) (p < 0.001), and SF-36 Physical Component Summary from 43.78 (9.46) to 48.79 (9.00) (p < 0.001). All these improvements were maintained until last follow-up. At 12-month follow-up and later, 52%-56% of evaluable patients (35%-42% of all patients) were improved by at least 50% of baseline CES-D scores. CES-D improved similarly in patients not using antidepressants or psychotherapy during the first six study months (55% of patients).
Conclusion: In outpatients with chronic depression, anthroposophic therapies were followed by long-term clinical improvement. Although the pre-post design of the present study does not allow for conclusions about comparative effectiveness, study findings suggest that the anthroposophic approach, with its recourse to non-verbal and artistic exercising therapies can be useful for patients motivated for such therapies.
Figures
Similar articles
-
Eurythmy therapy in chronic disease: a four-year prospective cohort study.BMC Public Health. 2007 Apr 23;7:61. doi: 10.1186/1471-2458-7-61. BMC Public Health. 2007. PMID: 17451596 Free PMC article.
-
Anthroposophic medical therapy in chronic disease: a four-year prospective cohort study.BMC Complement Altern Med. 2007 Apr 23;7:10. doi: 10.1186/1472-6882-7-10. BMC Complement Altern Med. 2007. PMID: 17451595 Free PMC article.
-
Anthroposophic therapies in chronic disease: the Anthroposophic Medicine Outcomes Study (AMOS).Eur J Med Res. 2004 Jul 30;9(7):351-60. Eur J Med Res. 2004. PMID: 15337636
-
Overview of the Publications From the Anthroposophic Medicine Outcomes Study (AMOS): A Whole System Evaluation Study.Glob Adv Health Med. 2014 Jan;3(1):54-70. doi: 10.7453/gahmj.2013.010. Glob Adv Health Med. 2014. PMID: 24753995 Free PMC article. Review.
-
Assessing the order of magnitude of outcomes in single-arm cohorts through systematic comparison with corresponding cohorts: an example from the AMOS study.BMC Med Res Methodol. 2008 Mar 19;8:11. doi: 10.1186/1471-2288-8-11. BMC Med Res Methodol. 2008. PMID: 18366683 Free PMC article. Review.
Cited by
-
Eurythmy Therapy in clinical studies: a systematic literature review.BMC Complement Altern Med. 2008 Mar 31;8:8. doi: 10.1186/1472-6882-8-8. BMC Complement Altern Med. 2008. PMID: 18377647 Free PMC article.
-
Anthroposophic therapy for migraine: a two-year prospective cohort study in routine outpatient settings.Open Neurol J. 2010;4:100-10. doi: 10.2174/1874205X01004010100. Epub 2010 Sep 8. Open Neurol J. 2010. PMID: 21673981 Free PMC article.
-
Anthroposophic medicine: an integrative medical system originating in europe.Glob Adv Health Med. 2013 Nov;2(6):20-31. doi: 10.7453/gahmj.2012.087. Glob Adv Health Med. 2013. PMID: 24416705 Free PMC article.
-
Efficacy of injections with Disci/Rhus toxicodendron compositum for chronic low back pain--a randomized placebo-controlled trial.PLoS One. 2011;6(11):e26166. doi: 10.1371/journal.pone.0026166. Epub 2011 Nov 8. PLoS One. 2011. PMID: 22087222 Free PMC article. Clinical Trial.
-
Predictors of outcome after 6 and 12 months following anthroposophic therapy for adult outpatients with chronic disease: a secondary analysis from a prospective observational study.BMC Res Notes. 2010 Aug 3;3:218. doi: 10.1186/1756-0500-3-218. BMC Res Notes. 2010. PMID: 20682028 Free PMC article.
References
-
- Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry. 1997;170:205–228. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
