

Neck ligament strength is decreased following whiplash trauma
- PMID: 17184536
- PMCID: PMC1764743
- DOI: 10.1186/1471-2474-7-103
Neck ligament strength is decreased following whiplash trauma
Abstract
Background: Previous clinical studies have documented successful neck pain relief in whiplash patients using nerve block and radiofrequency ablation of facet joint afferents, including capsular ligament nerves. No previous study has documented injuries to the neck ligaments as determined by altered dynamic mechanical properties due to whiplash. The goal of the present study was to determine the dynamic mechanical properties of whiplash-exposed human cervical spine ligaments. Additionally, the present data were compared to previously reported control data. The ligaments included the anterior and posterior longitudinal, capsular, and interspinous and supraspinous ligaments, middle-third disc, and ligamentum flavum.
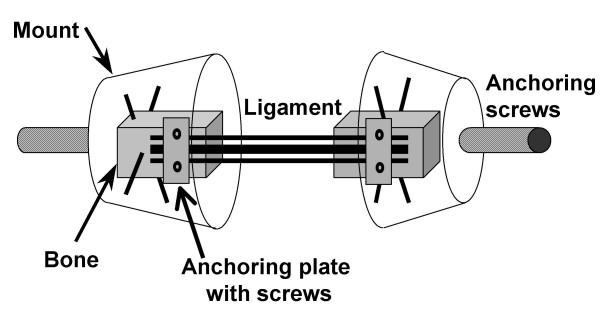
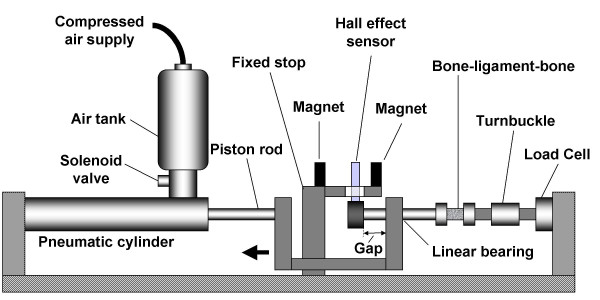
Methods: A total of 98 bone-ligament-bone specimens (C2-C3 to C7-T1) were prepared from six cervical spines following 3.5, 5, 6.5, and 8 g rear impacts and pre- and post-impact flexibility testing. The specimens were elongated to failure at a peak rate of 725 (SD 95) mm/s. Failure force, elongation, and energy absorbed, as well as stiffness were determined. The mechanical properties were statistically compared among ligaments, and to the control data (significance level: P < 0.05; trend: P < 0.1). The average physiological ligament elongation was determined using a mathematical model.
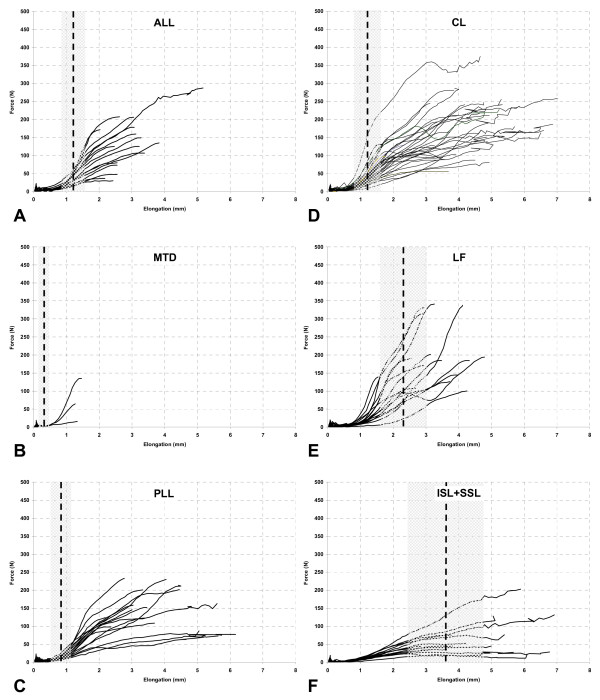
Results: For all whiplash-exposed ligaments, the average failure elongation exceeded the average physiological elongation. The highest average failure force of 204.6 N was observed in the ligamentum flavum, significantly greater than in middle-third disc and interspinous and supraspinous ligaments. The highest average failure elongation of 4.9 mm was observed in the interspinous and supraspinous ligaments, significantly greater than in the anterior longitudinal ligament, middle-third disc, and ligamentum flavum. The average energy absorbed ranged from 0.04 J by the middle-third disc to 0.44 J by the capsular ligament. The ligamentum flavum was the stiffest ligament, while the interspinous and supraspinous ligaments were most flexible. The whiplash-exposed ligaments had significantly lower (P = 0.036) failure force, 149.4 vs. 186.0 N, and a trend (P = 0.078) towards less energy absorption capacity, 308.6 vs. 397.0 J, as compared to the control data.
Conclusion: The present decreases in neck ligament strength due to whiplash provide support for the ligament-injury hypothesis of whiplash syndrome.
Figures
Similar articles
-
Dynamic mechanical properties of intact human cervical spine ligaments.Spine J. 2007 Nov-Dec;7(6):659-65. doi: 10.1016/j.spinee.2006.10.014. Epub 2007 Jan 2. Spine J. 2007. PMID: 17998125 Free PMC article.
-
Whiplash causes increased laxity of cervical capsular ligament.Clin Biomech (Bristol). 2008 Feb;23(2):159-65. doi: 10.1016/j.clinbiomech.2007.09.003. Epub 2007 Oct 23. Clin Biomech (Bristol). 2008. PMID: 17959284 Free PMC article.
-
Cervical facet capsular ligament yield defines the threshold for injury and persistent joint-mediated neck pain.J Biomech. 2007;40(10):2299-306. doi: 10.1016/j.jbiomech.2006.10.015. Epub 2006 Dec 1. J Biomech. 2007. PMID: 17141249
-
Three-column ligamentous extension injury of the thoracic spine: a case report and review of the literature.Spine (Phila Pa 1976). 2007 Dec 1;32(25):E785-8. doi: 10.1097/BRS.0b013e31815b60fd. Spine (Phila Pa 1976). 2007. PMID: 18245995 Review.
-
[Biomechanics of whiplash injury].Orthopade. 1998 Dec;27(12):813-9. doi: 10.1007/PL00003468. Orthopade. 1998. PMID: 9894235 Review. German.
Cited by
-
The effects of ligamentous injury in the human lower cervical spine.J Biomech. 2012 Oct 11;45(15):2668-72. doi: 10.1016/j.jbiomech.2012.08.012. Epub 2012 Aug 30. J Biomech. 2012. PMID: 22939289 Free PMC article.
-
Addition of lateral bending range of motion measurement to standard sagittal measurement to improve diagnosis sensitivity of ligamentous injury in the human lower cervical spine.Eur Spine J. 2016 Jan;25(1):122-126. doi: 10.1007/s00586-015-4110-z. Epub 2015 Jul 11. Eur Spine J. 2016. PMID: 26162921 Free PMC article.
-
Collagen organization regulates stretch-initiated pain-related neuronal signals in vitro: Implications for structure-function relationships in innervated ligaments.J Orthop Res. 2018 Feb;36(2):770-777. doi: 10.1002/jor.23657. Epub 2017 Aug 11. J Orthop Res. 2018. PMID: 28722281 Free PMC article.
-
Diagnostic Accuracy of Videofluoroscopy for Symptomatic Cervical Spine Injury Following Whiplash Trauma.Int J Environ Res Public Health. 2020 Mar 5;17(5):1693. doi: 10.3390/ijerph17051693. Int J Environ Res Public Health. 2020. PMID: 32150926 Free PMC article.
-
A Novel Radiological Scoring System for Anterior Longitudinal Ligament Injuries.Int J Gen Med. 2024 Feb 29;17:725-738. doi: 10.2147/IJGM.S446004. eCollection 2024. Int J Gen Med. 2024. PMID: 38481615 Free PMC article.
References
-
- Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, Zeiss E. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: redefining "whiplash" and its management. Spine. 1995;20:1S–73S. - PubMed
-
- Kasch H, Bach FW, Jensen TS. Handicap after acute whiplash injury: a 1-year prospective study of risk factors. Neurology. 2001;56:1637–1643. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
