

Coronary arterial fistulas
- PMID: 17184545
- PMCID: PMC1764722
- DOI: 10.1186/1750-1172-1-51
Coronary arterial fistulas
Abstract
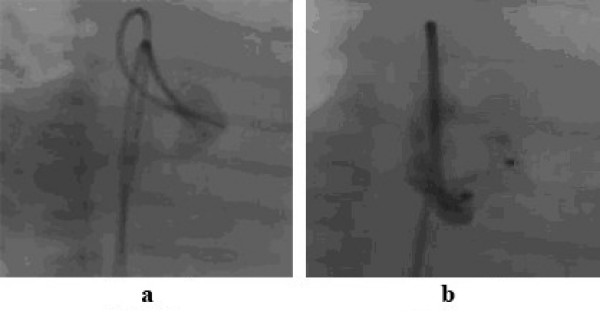
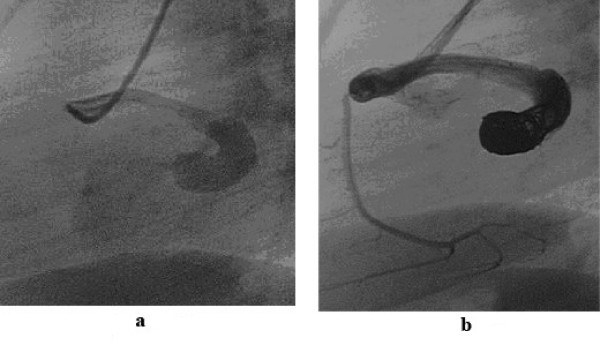
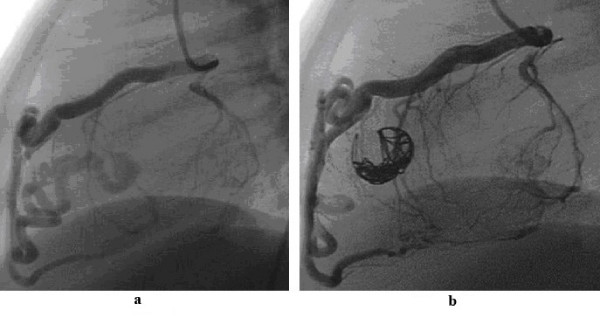
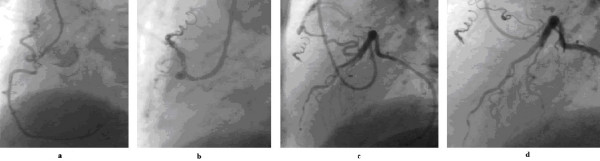
A coronary arterial fistula is a connection between one or more of the coronary arteries and a cardiac chamber or great vessel. This is a rare defect and usually occurs in isolation. Its exact incidence is unknown. The majority of these fistulas are congenital in origin although they may occasionally be detected after cardiac surgery. They do not usually cause symptoms or complications in the first two decades, especially when small. After this age, the frequency of both symptoms and complications increases. Complications include 'steal' from the adjacent myocardium, thrombosis and embolism, cardiac failure, atrial fibrillation, rupture, endocarditis/endarteritis and arrhythmias. Thrombosis within the fistula is rare but may cause acute myocardial infarction, paroxysmal atrial fibrillation and ventricular arrhythmias. Spontaneous rupture of the aneurysmal fistula causing haemopericardium has also been reported. The main differential diagnosis is patent arterial duct, although other congenital arteriovenous shunts need to be excluded. Whilst two-dimensional echocardiography helps to differentiate between the different shunts, coronary angiography is the main diagnostic tool for the delineation of the anatomy. Surgery was the traditional method of treatment but nowadays catheter closure is recommended using a variety of closure devices, such as coils, or other devices. With the catheter technique, the results are excellent with infrequent complications.
Figures
References
-
- Reidy JF, Anjos RT, Qureshi SA, Baker EJ, Tynan MJ. Transcatheter embolization in the treatment of coronary artery fistulas. J Am Coll Cardiol. 1991;18:187–192. - PubMed
-
- McNamara JJ, Gross RE. Congenital coronary artery fistula. Surgery. 1969;65:59–69. - PubMed
-
- Levin DC, Fellows KE, Abrams HL. Hemodynamically significant primary anomalies of the coronary arteries. Circulation. 1978;58:25–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
