

A case study of gait compensations for hip muscle weakness in idiopathic inflammatory myopathy
- PMID: 17187908
- PMCID: PMC1817673
- DOI: 10.1016/j.clinbiomech.2006.11.002
A case study of gait compensations for hip muscle weakness in idiopathic inflammatory myopathy
Abstract
Background: The purpose of this case series was to quantify different strategies used to compensate in gait for hip muscle weakness.
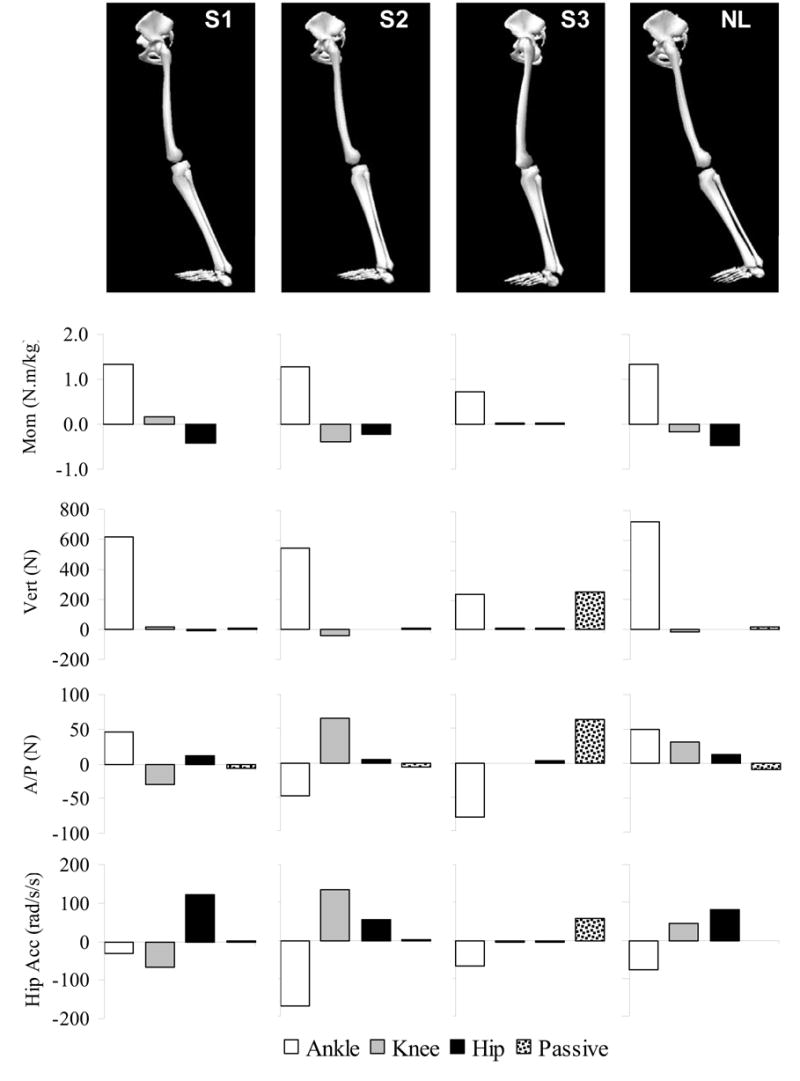
Methods: An instrumented gait analysis was performed of three females diagnosed with idiopathic inflammatory myopathies and compared to a healthy unimpaired subject. Lower extremity joint moments obtained from the gait analysis were used to drive an induced acceleration model which determined each moment's contribution to upright support, forward progression, and hip joint acceleration.
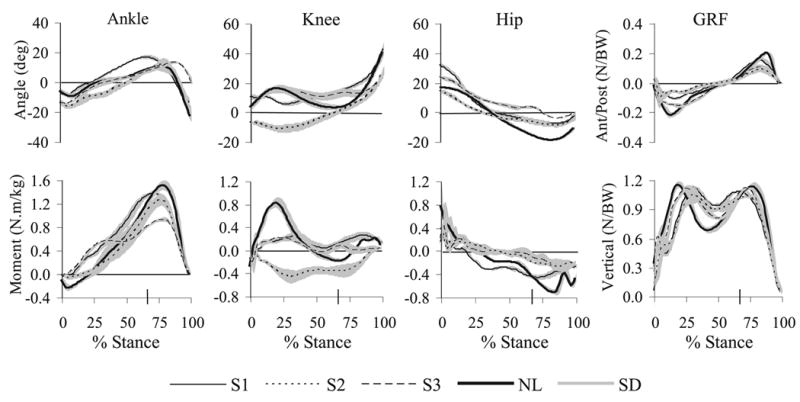
Findings: Results showed that after midstance, the ankle plantar flexors normally provide upright support and forward progression while producing hip extension acceleration. In normal gait, the hip flexors eccentrically resist hip extension, but the hip flexor muscles of the impaired subjects (S1-3) were too weak to control extension. Instead S1-3 altered joint positions and muscle function to produce forward progression while minimizing hip extension acceleration. S1 increased knee flexion angle to decrease the hip extension effect of the ankle plantar flexors. S2 and S3 used either a knee flexor moment or gravity to produce forward progression, which had the advantage of accelerating the hip into flexion rather than extension, and decreased the demand on the hip flexors.
Interpretation: Results showed how gait compensations for hip muscle weakness can produce independent (i.e. successful) ambulation, although at a reduced speed as compared to normal gait. Knowledge of these successful strategies can assist the rehabilitation of patients with hip muscle weakness who are unable to ambulate and potentially be used to reduce their disability.
Figures
References
-
- Amato AA, Barohn J. Idiopathic inflammatory myopathies. Neurologic Clinics. 1997;15:615–648. - PubMed
-
- Anderson FC, Pandy MG. Individual muscle contributions to support in normal walking. Gait & Posture. 2003;17:159–169. - PubMed
-
- Armand S, Mercier M, Watelain E, Patte K, Pelissier J, Rivier F. A comparison of gait in spinal muscular atrophy, type II and Duchenne muscular dystrophy. Gait & Posture. 2005;21:369–378. - PubMed
-
- Bohan A, Peter JB, Bowman RL, Pearson CM. Computer-assisted analysis of 153 patients with polymyositis and dermatomyositis. Medicine. 1977;56:255–286. - PubMed
-
- Bohannon RW. Strength of lower limb related to gait velocity and cadence in stroke patients. Physiotherapy Canada. 1986;38:204–206.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
