

Randomized effectiveness study of four therapeutic strategies for TMJ closed lock
- PMID: 17189464
- PMCID: PMC2278036
- DOI: 10.1177/154405910708600109
Randomized effectiveness study of four therapeutic strategies for TMJ closed lock
Erratum in
- J Dent Res. 2013 Jan;92(1):98
Abstract
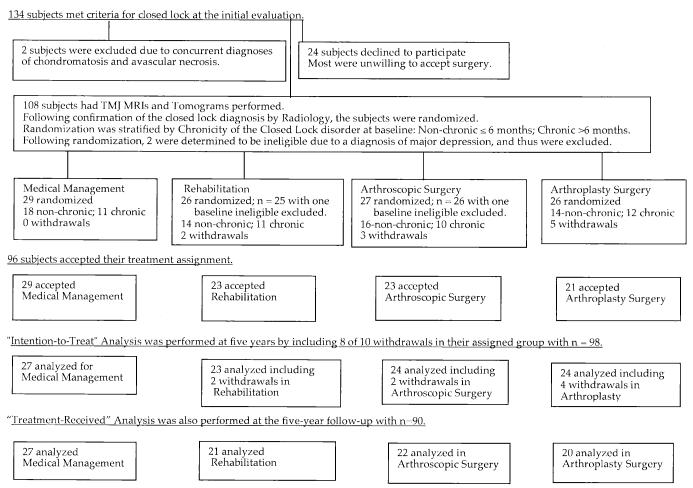
For individuals with temporomandibular joint (TMJ) disc displacement without reduction with limited mouth opening (closed lock), interventions vary from minimal treatment to surgery. In a single-blind trial, 106 individuals with TMJ closed lock were randomized among medical management, rehabilitation, arthroscopic surgery with post-operative rehabilitation, or arthroplasty with post-operative rehabilitation. Evaluations at baseline, 3, 6, 12, 18, 24, and 60 months used the Craniomandibular Index (CMI) and Symptom Severity Index (SSI) for jaw function and TMJ pain respectively. Using an intention-to-treat analysis, we observed no between-group difference at any follow-up for CMI (p > or = 0.33) or SSI (p > or = 0.08). Both outcomes showed within-group improvement (p < 0.0001) for all groups. The findings of this study suggest that primary treatment for individuals with TMJ closed lock should consist of medical management or rehabilitation. The use of this approach will avoid unnecessary surgical procedures.
Figures
Comment in
-
Non-surgical care should be the primary treatment for TMJ closed lock. Does medical management improve pain and jaw function as much and as quickly as rehabilitation with/ without surgery in the initial management of temporomandibular joint closed lock?Evid Based Dent. 2007;8(4):112. doi: 10.1038/sj.ebd.6400529. Evid Based Dent. 2007. PMID: 18158548 No abstract available.
-
TMJ closed lock symptoms improve, regardless of intervention.J Evid Based Dent Pract. 2008 Mar;8(1):19-21. doi: 10.1016/j.jebdp.2007.12.005. J Evid Based Dent Pract. 2008. PMID: 18346697 No abstract available.
-
Importance of time as a factor in the management of temporomandibular joint closed lock.Int J Oral Maxillofac Surg. 2014 Oct;43(10):1302-3. doi: 10.1016/j.ijom.2014.07.003. Epub 2014 Jul 25. Int J Oral Maxillofac Surg. 2014. PMID: 25069852 No abstract available.
-
Response to letter to the editor--Temporomandibular joint closed lock.Int J Oral Maxillofac Surg. 2014 Oct;43(10):1303-4. doi: 10.1016/j.ijom.2014.07.002. Epub 2014 Jul 25. Int J Oral Maxillofac Surg. 2014. PMID: 25069853 No abstract available.
References
APPENDIX REFERENCES
-
- Anderson GC, Schulte JK, Goodkind RJ. Comparative study of two treatment methods for internal derangement of the temporomandibular joint. J Prosthet Dent. 1985;53:392–397. - PubMed
-
- Azrin NH, Nunn RG. Habit-reversal: a method of eliminating nervous habits and tics. Behav Res Ther. 1973;11:619–628. - PubMed
-
- Braun BL. The effect of physical therapy intervention on incisal opening after temporomandibular joint surgery. Oral Surg Oral Med Oral Pathol. 1987;64:544–548. - PubMed
-
- Dahlström L, Haraldson T. Bite plates and stabilization splints in mandibular dysfunction. A clinical and electromyographic comparison. Acta Odontol Scand. 1985;43:109–114. - PubMed
-
- Fricton JR, Hathaway KM, Bromaghim C. Interdisciplinary management of patients with TMJ and craniofacial pain: characteristics and outcome. J Craniomandib Disord. 1987;1:115–122. - PubMed
References
-
- Derogatis LR. SCL-90-R: administration, scoring and procedures manual-II for the revised version. Clinical Psychometric Research; Towson, MD: 1992.
-
- Dimitroulis G. The role of surgery in the management of disorders of the temporomandibular joint: a critical review of the literature. Int J Oral Maxillofac Surg. 2005;34(Part 2):231–237. - PubMed
-
- Drangsholt M, LeResche L. In: Temporomandibular disorder pain. In: Epidemiology of pain. Crombie IK, Croft PR, Linton SJ, LeResche L, Von Korff M, editors. IASP Press; Seattle: 1999. pp. 203–233.
-
- Fricton JR, Schiffman EL. Reliability of a craniomandibular index. J Dent Res. 1986;65:1359–1364. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
