

Non-surgical treatment of vaginal agenesis using a simplified version of Ingram's method
- PMID: 17191323
- PMCID: PMC2687834
- DOI: 10.3349/ymj.2006.47.6.892
Non-surgical treatment of vaginal agenesis using a simplified version of Ingram's method
Abstract
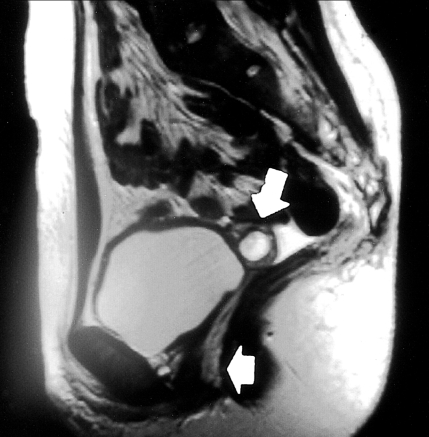
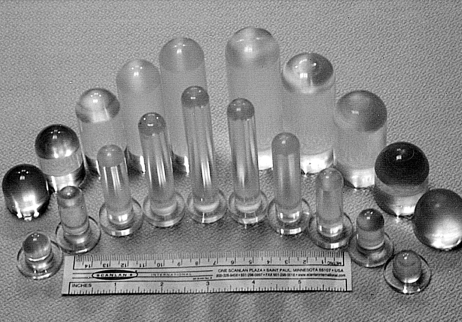
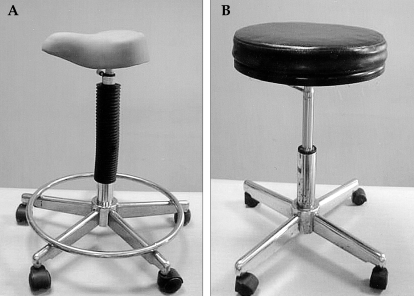
Non-surgical vaginal dilation is a safe and effective method for the creation of neovagina in the patient with vaginal agenesis. Compared to surgical methods, non-surgical vaginal dilation has the advantage of low morbidity, the creation of a more physiologic vaginal milieu, and no surgical scarring. To overcome some technical limitations of original Frank's method, in 1981 Ingram proposed a modification of the technique that used dilators of gradually increasing size mounted on a bicycle seat stool. Although several studies have shown satisfactory outcomes using Ingram's method, there are some practical difficulties in making and handling the bicycle seat stool. This article reports a case of a 24-year-old woman with Mayer-Rokitansky-Küster-Hauser syndrome whose vaginal agenesis is successfully treated with a simplified version of Ingram's method. This method uses dilators of gradually increasing size mounted on an ordinary chair instead of a bicycle seat stool. When necessary, the patient may use a fulcrum under the dilator.
Figures
Similar articles
-
An alternative approach to vaginal dilation in patients with Meyer-Rokitanski-Küster-Hauser syndrome: two case reports.Gynecol Endocrinol. 2020 Aug;36(8):746-748. doi: 10.1080/09513590.2020.1719061. Epub 2020 Jan 29. Gynecol Endocrinol. 2020. PMID: 31994956
-
Should progressive perineal dilation be considered first line therapy for vaginal agenesis?J Urol. 2009 Oct;182(4 Suppl):1882-9. doi: 10.1016/j.juro.2009.03.071. Epub 2009 Aug 20. J Urol. 2009. PMID: 19695600
-
Modification of the Ingram bicycle seat stool for the treatment of vaginal agenesis and stenosis.Int J Gynaecol Obstet. 2008 Sep;102(3):301-3. doi: 10.1016/j.ijgo.2008.04.018. Epub 2008 Jul 7. Int J Gynaecol Obstet. 2008. PMID: 18603249
-
Mayer-Rokitansky-Kuster-Hauser syndrome: complications, diagnosis and possible treatment options: a review.Gynecol Endocrinol. 2014 Sep;30(9):618-23. doi: 10.3109/09513590.2014.927855. Epub 2014 Jun 20. Gynecol Endocrinol. 2014. PMID: 24948340 Review.
-
Vaginal Dilator Therapy: A Guide for Providers for Assessing Readiness and Supporting Patients Through the Process Successfully.J Pediatr Adolesc Gynecol. 2019 Aug;32(4):354-358. doi: 10.1016/j.jpag.2019.05.002. Epub 2019 May 12. J Pediatr Adolesc Gynecol. 2019. PMID: 31091469 Review.
Cited by
-
Evaluation of vaginal agenesis treated with the modified McIndoe technique: A retrospective study.J Turk Ger Gynecol Assoc. 2016 Jan 12;17(2):101-5. doi: 10.5152/jtgga.2016.16013. eCollection 2016. J Turk Ger Gynecol Assoc. 2016. PMID: 27403077 Free PMC article.
-
Mayer-rokitansky-kuster-hauser syndrome: surgical management of two cases.J Surg Tech Case Rep. 2010 Jan;2(1):39-43. doi: 10.4103/2006-8808.63725. J Surg Tech Case Rep. 2010. PMID: 22091331 Free PMC article.
-
Recent advances in the molecular mechanisms of Mayer-Rokitansky-Küster-Hauser syndrome.Biomed Rep. 2017 Aug;7(2):123-127. doi: 10.3892/br.2017.929. Epub 2017 Jun 21. Biomed Rep. 2017. PMID: 28804623 Free PMC article.
-
Peritoneal vaginoplasty by Luohu I and Luohu II technique: a comparative study of the outcomes.Eur J Med Res. 2015 Aug 22;20(1):69. doi: 10.1186/s40001-015-0165-x. Eur J Med Res. 2015. Retraction in: Eur J Med Res. 2017 Aug 3;22(1):26. doi: 10.1186/s40001-017-0267-8. PMID: 26297245 Free PMC article. Retracted.
-
A Rare Case of Mayer-Rokitansky-Kuster-Hauser Syndrome Presenting with Acute Psychosis.J Clin Diagn Res. 2016 Apr;10(4):VD03-VD04. doi: 10.7860/JCDR/2016/18478.7658. Epub 2016 Apr 1. J Clin Diagn Res. 2016. PMID: 27190929 Free PMC article.
References
-
- Evans TN, Poland ML, Boving RL. Vaginal malformations. Am J Obstet Gynecol. 1981;141:910–920. - PubMed
-
- Frank RT. The formation of an artificial vagina without operation. Am J Obstet Gynecol. 1938;35:1053–1055.
-
- Roberts CP, Haber MJ, Rock JA. Vaginal creation for müllerian agenesis. Am J Obstet Gynecol. 2001;185:1349–1352. - PubMed
-
- Edmonds DK. Vaginal and uterine anomalies in the paediatric and adolescent patient. Curr Opin Obstet Gynecol. 2001;13:463–467. - PubMed
-
- Costa EM, Mendonca BB, Inacio M, Arnhold IJ, Silva FA, Lodovici O. Management of ambiguous genitalia in pseudohermaphrodites: new perspectives on vaginal dilation. Fertil Steril. 1997;67:229–232. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
