

Rifampicin/Cotrimoxazole/Isoniazid versus mefloquine or quinine + sulfadoxine- pyrimethamine for malaria: a randomized trial
- PMID: 17192794
- PMCID: PMC1713262
- DOI: 10.1371/journal.pctr.0010038
Rifampicin/Cotrimoxazole/Isoniazid versus mefloquine or quinine + sulfadoxine- pyrimethamine for malaria: a randomized trial
Abstract
Objectives: Previous studies of a fixed combination including cotrimoxazole, rifampicin, and isoniazid (Cotrifazid) showed efficacy against resistant strains of Plasmodium falciparum in animal models and in small-scale human studies. We conducted a multicentric noninferiority trial to assess the safety and efficacy of Cotrifazid against drug-resistant malaria in Papua New Guinea.
Design: The trial design was open-label, block-randomised, comparative, and multicentric.
Setting: The trial was conducted in four primary care health facilities, two in urban and two in rural areas of Madang and East Sepik Province, Papua New Guinea.
Participants: Patients of all ages with recurrent uncomplicated malaria were included.
Interventions: Patients were randomly assigned to receive Cotrifazid, mefloquine, or the standard treatment of quinine with sulfadoxine-pyrimethamine (SP).
Outcome measures: Incidence of clinical and laboratory adverse events and rate of clinical and/or parasitological failure at day 14 were recorded.
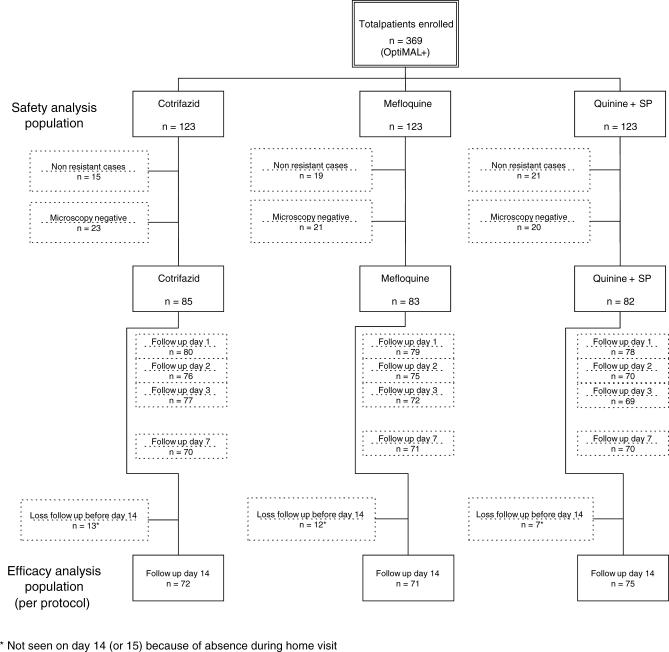
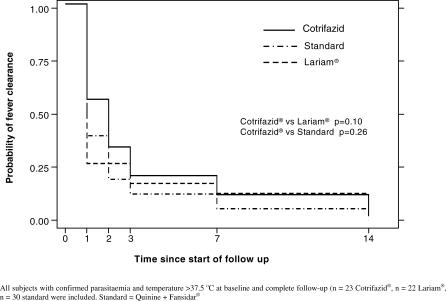
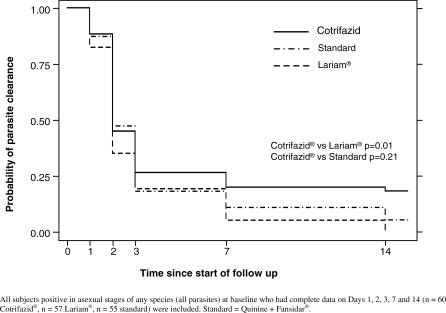
Results: The safety analysis population included 123 patients assigned to Cotrifazid, 123 to mefloquine, and 123 to quinine + SP. The Cotrifazid group experienced lower overall incidence of adverse events than the other groups. Among the efficacy analysis population (72 Cotrifazid, 71 mefloquine, and 75 quinine + SP), clinical failure rate (symptoms and parasite load) on day 14 was equivalent for the three groups (0% for Cotrifazid and mefloquine; 1% for quinine + SP), but parasitological failure rate (P. falciparum asexual blood-stage) was higher for Cotrifazid than for mefloquine or quinine + SP (9% [PCR corrected 8%] versus 0% and 3%, respectively [p = 0.02]).
Conclusion: Despite what appears to be short-term clinical equivalence, the notable parasitological failure at day 14 in both P. falciparum and P. vivax makes Cotrifazid in its current formulation and regimen a poor alternative combination therapy for malaria.
Conflict of interest statement
Figures
References
-
- Genton B, Baea K, Lorry K, Ginny M, Wines B, et al. Parasitological and clinical efficacy of standard treatment regimens against Plasmodium falciparum, P. vivax and P. malariae in Papua New Guinea. P N G Med J. 2005;48:141–150. - PubMed
-
- Alger NE, Spira DT, Silverman PH. Inhibition of rodent malaria in mice by rifampicin. Nature. 1970;227:381–382. - PubMed
-
- Bloland PB, Redd SC, Kazembe P, Tembenu R, Wirima JJ, et al. Co-trimoxazole for childhood febrile illness in malaria-endemic regions. Lancet. 1991;337:518–520. - PubMed
-
- Hutchinson DB, Farquhar JA. Trimethoprim-sulfamethoxazole in the treatment of malaria, toxoplasmosis, and pediculosis. Rev Infect Dis. 1982;4:419–425. - PubMed
LinkOut - more resources
Full Text Sources
