

Prostate biopsy: targeting cancer for detection and therapy
- PMID: 17192796
- PMCID: PMC1751027
Prostate biopsy: targeting cancer for detection and therapy
Abstract
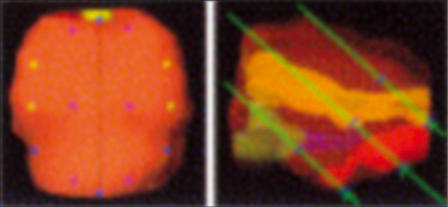
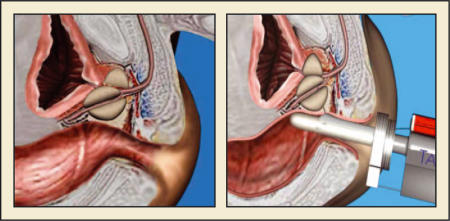
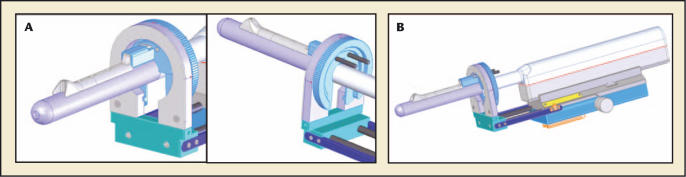
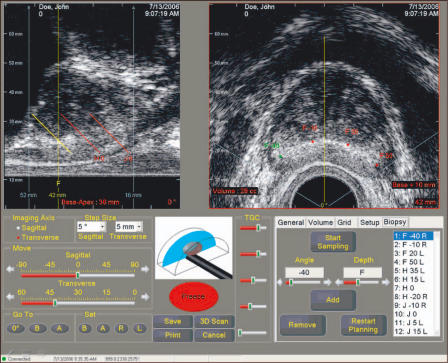
Despite improvements in cancer detection, prostate biopsy still lacks the ability to accurately map locations of cancer within the prostate. Improvements in prostate imaging may allow more accurate mapping of overall disease volume. Magnetic resonance (MR) spectroscopy allows improved specificity in detecting even small foci of disease within the peripheral zone. Improvements in MR-guided biopsy techniques may allow this technology to be adapted to therapeutics as well. Computer modeling of individual prostates serves as a means of designing optimized plans for prostate biopsy. The use of novel targeted biopsy schemes may allow an integration of available technologies in detection and localization of prostate cancer. Computer-directed needle biopsies based on anatomic landmarks within the prostate and computerized three-dimensional reconstruction of the gland may allow a highly reproducible means of identifying small foci of cancer, targeting them for therapy, and monitoring for recurrence. The TargetScan(R) system (Envisioneering Medical Technologies, St. Louis, MO) is the first technology to integrate available targeting methodologies in a systematic fashion.
Figures

Similar articles
-
Is there a better way to biopsy the prostate? Prospects for a novel transrectal systematic biopsy approach.Urology. 2007 Dec;70(6 Suppl):22-6. doi: 10.1016/j.urology.2007.06.1128. Urology. 2007. PMID: 18194707
-
Evaluation of a novel precision template-guided biopsy system for detecting prostate cancer.BJU Int. 2008 Aug 5;102(5):546-50. doi: 10.1111/j.1464-410X.2008.07832.x. BJU Int. 2008. PMID: 18694408
-
The eternal enigma in prostatic biopsy access route.Arch Ital Urol Androl. 2017 Oct 3;89(3):245-246. doi: 10.4081/aiua.2017.3.245. Arch Ital Urol Androl. 2017. PMID: 28969413
-
Targeted prostate biopsy and MR-guided therapy for prostate cancer.Abdom Radiol (NY). 2016 May;41(5):877-88. doi: 10.1007/s00261-016-0681-3. Abdom Radiol (NY). 2016. PMID: 26907717 Free PMC article. Review.
-
Multiparametric MRI and targeted prostate biopsy: Improvements in cancer detection, localization, and risk assessment.Cent European J Urol. 2016;69(1):9-18. doi: 10.5173/ceju.2016.734. Epub 2016 Jan 25. Cent European J Urol. 2016. PMID: 27123316 Free PMC article. Review.
Cited by
-
Diffusion weighted imaging in prostate cancer.Eur Radiol. 2011 Mar;21(3):593-603. doi: 10.1007/s00330-010-1960-y. Epub 2010 Oct 9. Eur Radiol. 2011. PMID: 20936413 Review.
-
Acoustic radiation force impulse imaging of human prostates ex vivo.Ultrasound Med Biol. 2010 Apr;36(4):576-88. doi: 10.1016/j.ultrasmedbio.2009.12.006. Ultrasound Med Biol. 2010. PMID: 20350685 Free PMC article.
-
Simulation of autonomous robotic multiple-core biopsy by 3D ultrasound guidance.Ultrason Imaging. 2010 Apr;32(2):118-27. doi: 10.1177/016173461003200205. Ultrason Imaging. 2010. PMID: 20687279 Free PMC article.
-
Pathology: the lottery of conventional prostate biopsy.Nat Rev Urol. 2009 Apr;6(4):188-9. doi: 10.1038/nrurol.2009.46. Nat Rev Urol. 2009. PMID: 19352393 No abstract available.
-
MR imaging of the prostate in clinical practice.MAGMA. 2008 Nov;21(6):379-92. doi: 10.1007/s10334-008-0138-y. Epub 2008 Sep 16. MAGMA. 2008. PMID: 18795354 Review.
References
-
- Roehl KA, Antenor JA, Catalona WJ. Serial biopsy results in prostate cancer screening study. J Urol. 2002;167:2435–2439. - PubMed
-
- Catalona WJ, Smith DS, Ratliff TL, et al. Measurement of prostate-specific antigen in serum as a screening test for prostate cancer. N Engl J Med. 1991;324:1156–1161. - PubMed
-
- Levine MA, Ittman M, Melamed J, Lepor H. Two consecutive sets of transrectal ultrasound guided sextant biopsies of the prostate for the detection of prostate cancer. J Urol. 1998;159:471–475. discussion 475–476. - PubMed
-
- Borboroglu PG, Comer SW, Riffenburgh RH, Amling CL. Extensive repeat transrectal ultrasound guided prostate biopsy in patients with previous benign sextant biopsies. J Urol. 2000;163:158–162. - PubMed
-
- Babaian RJ, Toi A, Kamoi K, et al. A comparative analysis of sextant and an extended 11-core multisite directed biopsy strategy. J Urol. 2000;163:152–157. - PubMed
LinkOut - more resources
Full Text Sources