

Children with severe malnutrition: can those at highest risk of death be identified with the WHO protocol?
- PMID: 17194194
- PMCID: PMC1716191
- DOI: 10.1371/journal.pmed.0030500
Children with severe malnutrition: can those at highest risk of death be identified with the WHO protocol?
Abstract
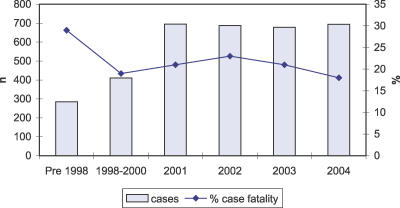
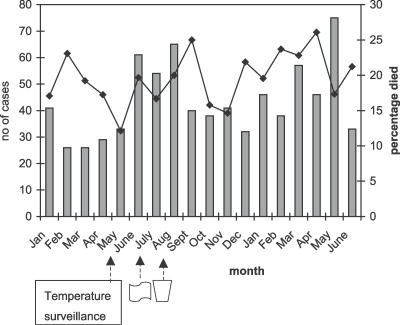
Background: With strict adherence to international recommended treatment guidelines, the case fatality for severe malnutrition ought to be less than 5%. In African hospitals, fatality rates of 20% are common and are often attributed to poor training and faulty case management. Improving outcome will depend upon the identification of those at greatest risk and targeting limited health resources. We retrospectively examined the major risk factors associated with early (<48 h) and late in-hospital death in children with severe malnutrition with the aim of identifying admission features that could distinguish a high-risk group in relation to the World Health Organization (WHO) guidelines.
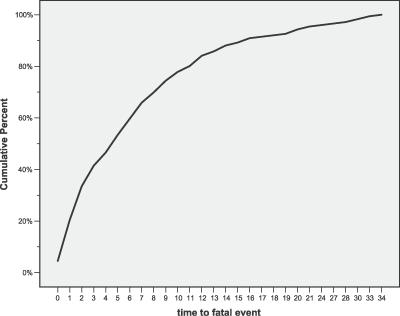
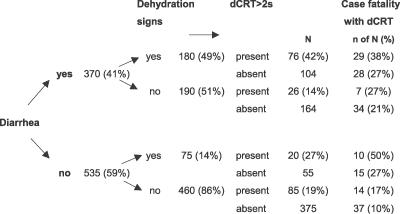
Methods and findings: Of 920 children in the study, 176 (19%) died, with 59 (33%) deaths occurring within 48 h of admission. Bacteraemia complicated 27% of all deaths: 52% died before 48 h despite 85% in vitro antibiotic susceptibility of cultured organisms. The sensitivity, specificity, and likelihood ratio of the WHO-recommended "danger signs" (lethargy, hypothermia, or hypoglycaemia) to predict early mortality was 52%, 84%, and 3.4% (95% confidence interval [CI] = 2.2 to 5.1), respectively. In addition, four bedside features were associated with early case fatality: bradycardia, capillary refill time greater than 2 s, weak pulse volume, and impaired consciousness level; the presence of two or more features was associated with an odds ratio of 9.6 (95% CI = 4.8 to 19) for early fatality (p < 0.0001). Conversely, the group of children without any of these seven features, or signs of dehydration, severe acidosis, or electrolyte derangements, had a low fatality (7%).
Conclusions: Formal assessment of these features as emergency signs to improve triage and to rationalize manpower resources toward the high-risk groups is required. In addition, basic clinical research is necessary to identify and test appropriate supportive treatments.
Conflict of interest statement
Figures
References
-
- Ashworth A, Khanum S, Jackson A, Schofield C. Guidelines for the inpatient treatment of severely malnourished children. New Delhi: World Health Organization Regional Office for South-East Asia; 2003. pp. 5–6.
-
- Ashworth A, Chopra M, McCoy D, Sanders D, Jackson D, et al. WHO guidelines for management of severe malnutrition in rural South African hospitals: Effect on case fatality and the influence of operational factors. Lancet. 2004;363:1110–1115. - PubMed
-
- Puoane T, Sanders D, Chopra M, Ashworth A, Strasser S, et al. Evaluating the clinical management of severely malnourished children—A study of two rural district hospitals. S Afr Med J. 2001;91:137–141. - PubMed
-
- Nathoo KJ, Bannerman CH, Pirie DJ. Pattern of admissions to the paediatric medical wards (1995 to 1996) at Harare Hospital, Zimbabwe. Cent Afr J Med. 1999;45:258–263. - PubMed
