

The cost of uncomplicated childhood fevers to Kenyan households: implications for reaching international access targets
- PMID: 17196105
- PMCID: PMC1770919
- DOI: 10.1186/1471-2458-6-314
The cost of uncomplicated childhood fevers to Kenyan households: implications for reaching international access targets
Abstract
Background: Fever is the clinical hallmark of malaria disease. The Roll Back Malaria (RBM) movement promotes prompt, effective treatment of childhood fevers as a key component to achieving its optimistic mortality reduction goals by 2010. A neglected concern is how communities will access these new medicines promptly and the costs to poor households when they are located in rural areas distant to health services.
Methods: We assemble data developed between 2001 and 2002 in Kenya to describe treatment choices made by rural households to treat a child's fever and the related costs to households. Using a cost-of-illness approach, we estimate the expected cost of a childhood fever to Kenyan households in 2002. We develop two scenarios to explore how expected costs to households would change if more children were treated at a health care facility with an effective antimalarial within 48 hours of fever onset.
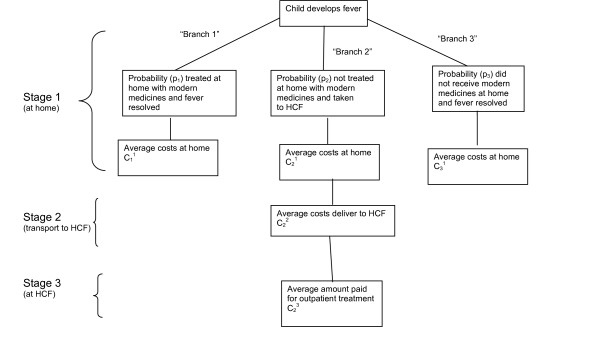
Results: 30% of uncomplicated fevers were managed at home with modern medicines, 38% were taken to a health care facility (HCF), and 32% were managed at home without the use of modern medicines. Direct household cash expenditures were estimated at $0.44 per fever, while the total expected cost to households (cash and time) of an uncomplicated childhood fever is estimated to be $1.91. An estimated mean of 1.42 days of caretaker time devoted to each fever accounts for the majority of household costs of managing fevers. The aggregate cost to Kenyan households of managing uncomplicated childhood fevers was at least $96 million in 2002, equivalent to 1.00% of the Kenyan GDP. Fewer than 8% of all fevers were treated with an antimalarial drug within 24 hours of fever onset, while 17.5% were treated within 48 hours at a HCF. To achieve an increase from 17.5% to 33% of fevers treated with an antimalarial drug within 48 hours at a HCF (Scenario 1), children already being taken to a HCF would need to be taken earlier. Under this scenario, direct cash expenditures would not change, and total household costs would fall slightly to $1.86 because caretakers also save time with prompt treatment if the child has malaria.
Conclusion: The management of uncomplicated childhood fevers imposes substantial costs on Kenyan households. Achieving substantial improvements in the numbers of fevers treated within 48 hours at a HCF with an effective antimalarial drug (Scenario 1) will not impose additional costs on households. Achieving additional improvements in fevers treated promptly at a HCF (Scenario 2) will impose additional costs on some households roughly equal to average cash expenses for transportation to a HCF. Additional financing mechanisms that further reduce the costs of accessing care at a HCF and/or that make artemisinin-based combination therapies (ACTs) accessible for home management need to be developed and evaluated as a top priority.
Figures
Similar articles
-
The impact of retail-sector delivery of artemether-lumefantrine on malaria treatment of children under five in Kenya: a cluster randomized controlled trial.PLoS Med. 2011 May;8(5):e1000437. doi: 10.1371/journal.pmed.1000437. Epub 2011 May 31. PLoS Med. 2011. PMID: 21655317 Free PMC article. Clinical Trial.
-
Access to subsidized artemether-lumefantrine from the private sector among febrile children in rural setting in Kilosa, Tanzania.Tanzan J Health Res. 2012 Apr;14(2):89-95. doi: 10.4314/thrb.v14i2.1. Tanzan J Health Res. 2012. PMID: 26591729
-
Accessibility, availability and affordability of anti-malarials in a rural district in Kenya after implementation of a national subsidy scheme.Malar J. 2011 Oct 26;10:316. doi: 10.1186/1475-2875-10-316. Malar J. 2011. PMID: 22029829 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Artemisinin-based combinations.Curr Opin Infect Dis. 2005 Dec;18(6):531-6. doi: 10.1097/01.qco.0000186848.46417.6c. Curr Opin Infect Dis. 2005. PMID: 16258328 Review.
Cited by
-
Insights into the Affordable Medicines Facility-malaria in Ghana: the role of caregivers and licensed chemical sellers in four regions.Malar J. 2016 May 10;15(1):263. doi: 10.1186/s12936-016-1307-5. Malar J. 2016. PMID: 27160685 Free PMC article.
-
The economic burden of inpatient paediatric care in Kenya: household and provider costs for treatment of pneumonia, malaria and meningitis.Cost Eff Resour Alloc. 2009 Jan 22;7:3. doi: 10.1186/1478-7547-7-3. Cost Eff Resour Alloc. 2009. PMID: 19161598 Free PMC article.
-
Assessment of health benefits and cost-effectiveness of 10-valent and 13-valent pneumococcal conjugate vaccination in Kenyan children.PLoS One. 2013 Jun 24;8(6):e67324. doi: 10.1371/journal.pone.0067324. Print 2013. PLoS One. 2013. PMID: 23826268 Free PMC article.
-
A framework for evaluating the costs of malaria elimination interventions: an application to reactive case detection in Southern Province of Zambia, 2014.Malar J. 2016 Aug 11;15(1):408. doi: 10.1186/s12936-016-1457-5. Malar J. 2016. PMID: 27515533 Free PMC article.
-
The quest for universal access to effective malaria treatment: how can the AMFm contribute?Malar J. 2010 Oct 8;9:274. doi: 10.1186/1475-2875-9-274. Malar J. 2010. PMID: 20932286 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
