

p66 Shc and tyrosine-phosphorylated Shc in primary breast tumors identify patients likely to relapse despite tamoxifen therapy
- PMID: 17196107
- PMCID: PMC1797038
- DOI: 10.1186/bcr1631
p66 Shc and tyrosine-phosphorylated Shc in primary breast tumors identify patients likely to relapse despite tamoxifen therapy
Abstract
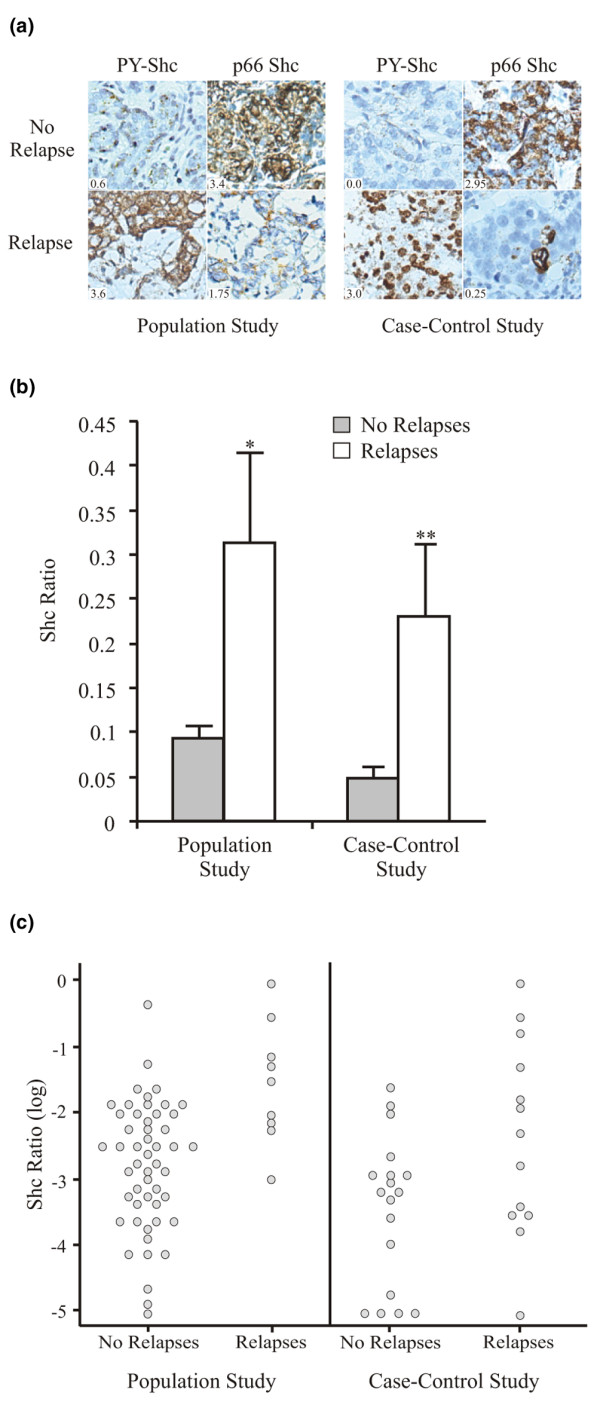
Introduction: Shc adapter proteins are secondary messenger proteins involved in various cellular pathways, including those mediating receptor tyrosine kinase signaling and apoptosis in response to stress. We have previously reported that high levels of tyrosine-phosphorylated Shc (PY-Shc) and low levels of its inhibitory p66 Shc isoform are strongly prognostic for identifying both early node-negative and more advanced, node-positive, primary breast cancers with high risk for recurrence. Because aberrant activation of tyrosine kinases upstream of Shc signaling proteins has been implicated in resistance to tamoxifen--the most widely prescribed drug for treatment of estrogen receptor-positive breast cancer--we hypothesized that Shc isoforms may identify patients at increased risk of relapsing despite tamoxifen treatment.
Methods: Immunohistochemical analyses of PY-Shc and p66 Shc were performed on archival primary breast cancer tumors from a population-based cohort (60 patients, 9 relapses) and, for validation, an independent external cohort (31 patients, 13 relapses) in which all patients received tamoxifen as a sole systemic adjuvant prior to relapse.
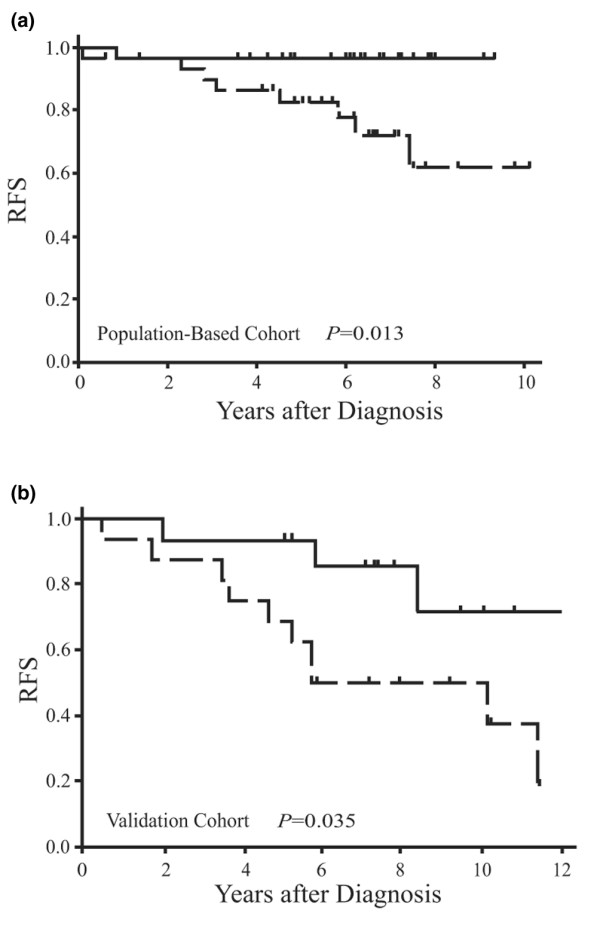
Results: By univariate and multivariate analyses, the Shc proteins were very strong and independent predictors of treatment failure in both the population-based cohort (interquartile hazard ratio = 8.3, 95% confidence interval [CI] 1.8 to 38, P = 0.007) and the validating cohort (interquartile relative risk = 12.1, 95% CI 1.7 to 86, P = 0.013).
Conclusion: These results suggest that the levels of PY-Shc and p66 Shc proteins in primary tumors identify patients at high risk for relapsing despite treatment with tamoxifen and therefore with further validation may be useful in guiding clinicians to select alternative adjuvant treatment strategies.
Figures
Similar articles
-
Shc proteins are strong, independent prognostic markers for both node-negative and node-positive primary breast cancer.Cancer Res. 2003 Oct 15;63(20):6772-83. Cancer Res. 2003. PMID: 14583473
-
Constitutively tyrosine phosphorylated p52 Shc in breast cancer cells: correlation with ErbB2 and p66 Shc expression.Breast Cancer Res Treat. 1998 May;49(2):119-28. doi: 10.1023/a:1006007227747. Breast Cancer Res Treat. 1998. PMID: 9696394
-
p66 Shc tumor levels show a strong prognostic correlation with disease outcome in stage IIA colon cancer.Clin Cancer Res. 2007 Oct 1;13(19):5798-804. doi: 10.1158/1078-0432.CCR-07-0073. Clin Cancer Res. 2007. PMID: 17908971
-
p66(Shc): at the crossroad of oxidative stress and the genetics of aging.Trends Mol Med. 2003 May;9(5):206-10. doi: 10.1016/s1471-4914(03)00048-0. Trends Mol Med. 2003. PMID: 12763525 Review.
-
[Regulatory effects of Shc-related phosphotyrosine adaptor proteins on aging].Yao Xue Xue Bao. 2008 Aug;43(8):793-800. Yao Xue Xue Bao. 2008. PMID: 18956770 Review. Chinese.
Cited by
-
ShcA signalling is essential for tumour progression in mouse models of human breast cancer.EMBO J. 2008 Mar 19;27(6):910-20. doi: 10.1038/emboj.2008.22. Epub 2008 Feb 14. EMBO J. 2008. PMID: 18273058 Free PMC article.
-
The adaptor proteins p66Shc and Grb2 regulate the activation of the GTPases ARF1 and ARF6 in invasive breast cancer cells.J Biol Chem. 2014 Feb 28;289(9):5687-703. doi: 10.1074/jbc.M113.516047. Epub 2014 Jan 9. J Biol Chem. 2014. PMID: 24407288 Free PMC article.
-
D,L-sulforaphane-induced apoptosis in human breast cancer cells is regulated by the adapter protein p66Shc.J Cell Biochem. 2012 Feb;113(2):599-610. doi: 10.1002/jcb.23386. J Cell Biochem. 2012. PMID: 21956685 Free PMC article.
-
Can pharmacological receptor tyrosine kinase inhibitors sensitize poor outcome breast tumors to immune-based therapies?Front Oncol. 2013 Feb 13;3:23. doi: 10.3389/fonc.2013.00023. eCollection 2013. Front Oncol. 2013. PMID: 23408142 Free PMC article.
-
Oxidative Stress in Breast Cancer: A Biochemical Map of Reactive Oxygen Species Production.Curr Issues Mol Biol. 2024 May 13;46(5):4646-4687. doi: 10.3390/cimb46050282. Curr Issues Mol Biol. 2024. PMID: 38785550 Free PMC article. Review.
References
-
- Hayes DF. Tamoxifen: Dr. Jekyll and Mr. Hyde? J Natl Cancer Inst. 2004;96:895–897. - PubMed
-
- Jaiyesimi IA, Buzdar AU, Decker DA, Hortobagyi GN. Use of tamoxifen for breast cancer: twenty-eight years later. J Clin Oncol. 1995;13:513–529. - PubMed
-
- Shou J, Massarweh S, Osborne CK, Wakeling AE, Ali S, Weiss H, Schiff R. Mechanisms of tamoxifen resistance: increased estrogen receptor-HER2/neu cross-talk in ER/HER2-positive breast cancer. J Natl Cancer Inst. 2004;96:926–935. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
