

Using cost-effectiveness analyses to inform policy: the case of antiretroviral therapy in Thailand
- PMID: 17196110
- PMCID: PMC1779364
- DOI: 10.1186/1478-7547-4-21
Using cost-effectiveness analyses to inform policy: the case of antiretroviral therapy in Thailand
Abstract
Background: Much emphasis is put on providing evidence to assist policymakers in priority setting and investment decisions. Assessing the cost-effectiveness of interventions is one technique used by policymakers in their decisions around the allocation of scarce resources. However, even where such evidence is available, other considerations may also be taken into account, and even over-ride technical evidence. Antiretroviral therapy (ART) is the most effective intervention to reduce HIV-related morbidity and prolong mortality. However, treatment provision in the developing world has been hindered by the high costs of services and drugs, casting doubts on its cost-effectiveness. This paper looks at Thailand's publicly-funded antiretroviral initiative which was first introduced in 1992, and explores the extent to which cost-effectiveness evidence influenced policy.
Methods: This article reviews the development of the national ART programme in Thailand between 1992 and 2004. It examines the roles of cost-effectiveness information in treatment policy decisions. Qualitative approaches including document analysis and interview of key informants were employed.
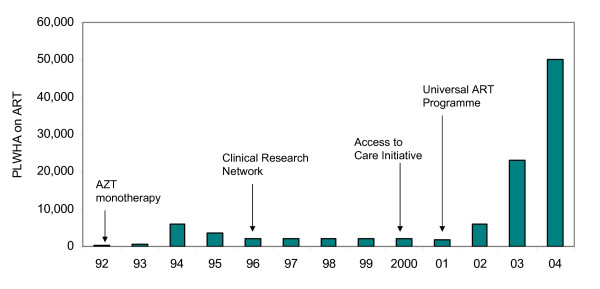
Results: Two significant policy shifts have been observed in government-organised ART provision. In 1996, service-based therapy for a few was replaced by a research network to support clinical assessments of antiretroviral medication in public hospitals. This decision was taken after a domestic study illustrated the unaffordable fiscal burden and inefficient use of resources in provision of ART. The numbers of treatment recipients was maintained at 2,000 per year throughout the 1990s. It was not until 2001 that a new government pledged to extend the numbers receiving the service, as part of its commitment to universal coverage. Several elements played a role in this decision: new groups of dominant actors, drug price reductions, a pro-active civil society movement, lessons from experience on treatment benefits, and global treatment advocacy. Unlike previous policy discourse, human rights, ethics and equity notions were explicitly raised to support therapy extension.
Conclusion: In the early decision, moving from a relatively limited ART service to a research network was clearly influenced by cost-effectiveness data. But in the 2001 decision to include ART in the universal coverage package, cost-effectiveness arguments were over-ruled by other considerations. Thai ART policy was shaped by many factors, and was not a simple rational process which relied on evidence.
Figures
Similar articles
-
The economics of effective AIDS treatment in Thailand.AIDS. 2007 Jul;21 Suppl 4:S105-16. doi: 10.1097/01.aids.0000279713.39675.1c. AIDS. 2007. PMID: 17620745
-
The Economic Impact of Smoking and of Reducing Smoking Prevalence: Review of Evidence.Tob Use Insights. 2015 Jul 14;8:1-35. doi: 10.4137/TUI.S15628. eCollection 2015. Tob Use Insights. 2015. PMID: 26242225 Free PMC article. Review.
-
Procedural fairness in benefit package design: inclusion of pre-exposure prophylaxis of HIV in Universal Coverage Scheme in Thailand.Health Policy Plan. 2023 Nov 14;38(Supplement_1):i36-i48. doi: 10.1093/heapol/czad061. Health Policy Plan. 2023. PMID: 37963082 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Strengthening cost-effectiveness analysis in Thailand through the establishment of the health intervention and technology assessment program.Pharmacoeconomics. 2009;27(11):931-45. doi: 10.2165/11314710-000000000-00000. Pharmacoeconomics. 2009. PMID: 19888793 Review.
Cited by
-
Health technology assessment and its role in the future development of the Indian healthcare sector.Perspect Clin Res. 2012 Apr;3(2):66-72. doi: 10.4103/2229-3485.96449. Perspect Clin Res. 2012. PMID: 22701823 Free PMC article.
-
Government use licenses in Thailand: The power of evidence, civil movement and political leadership.Global Health. 2011 Sep 12;7:32. doi: 10.1186/1744-8603-7-32. Global Health. 2011. PMID: 21910864 Free PMC article.
-
S4HARA: System for HIV/AIDS resource allocation.Cost Eff Resour Alloc. 2008 Mar 26;6:7. doi: 10.1186/1478-7547-6-7. Cost Eff Resour Alloc. 2008. PMID: 18366800 Free PMC article.
-
Multi-criteria decision analysis for setting priorities on HIV/AIDS interventions in Thailand.Health Res Policy Syst. 2012 Feb 17;10:6. doi: 10.1186/1478-4505-10-6. Health Res Policy Syst. 2012. PMID: 22339981 Free PMC article.
-
Mortality and treatment costs of hospitalized chronic kidney disease patients between the three major health insurance schemes in Thailand.BMC Health Serv Res. 2016 Sep 29;16(1):528. doi: 10.1186/s12913-016-1792-9. BMC Health Serv Res. 2016. PMID: 27686066 Free PMC article.
References
-
- WHO/UNAIDS . Progress on Global Access to HIV Antiretroviral Therapy: A Report on "3 by 5" and Beyond, March 2006. Geneva ; 2006.
-
- Kumaranayake L. Economies of scale-up? The cost of expanding access http://www.id21.org/insights/insights-h02/insights-issh02-art05.html
Grants and funding
LinkOut - more resources
Full Text Sources
